The risk of permanent disability or death from the MMR vaccine may be greater than the risk posed by measles, mumps or rubella infection because large enough vaccine safety studies haven’t been done, according to a collection of new documents released by Physicians for Informed Consent (PIC).
The collection includes disease information statements for measles, mumps and rubella, and a vaccine risk statement for the MMR vaccine.
According to the Mayo Clinic, measles is a viral infection typically accompanied by a skin rash, fever, cough, runny nose, sore throat, inflamed eyes and tiny white spots on the inner cheek.
Mumps and rubella also are viral infections. According to PIC, all three viral infections typically resolve on their own with proper rest and hydration in almost all cases.
Dr. Shira Miller, PIC’s founder and president, told The Defender, “The main takeaway is that the MMR vaccine has not been proven safer than measles, mumps and rubella.”
PIC is a nonprofit that delivers data to doctors and the public so they can “evaluate the data on infectious diseases and vaccines objectively, and voluntarily engage in informed decision-making about vaccination.”
Miller explained that the MMR vaccine clinical trials didn’t include enough subjects to be able to prove that the risk of permanent disability or death from the vaccine is less than the risk of permanent disability or death from measles, mumps or rubella.
The number of measles, mumps or rubella infections that result in permanent disability or death is so low that researchers would need to have at least 50,000 subjects in a clinical trial to be able to show that the vaccine is safer than the disease.
The MMR vaccine’s clinical trials fall very short of that benchmark, according to PIC’s statement on MMR vaccine risk.
Prelicensure clinical trials for vaccines, including the MMR shot, are “relatively small and usually last no longer than a few years,” according to the Centers for Disease Control and Prevention’s (CDC) 2024 “Manual for the Surveillance of Vaccine-Preventable Diseases.”
The 2024 edition of the CDC manual doesn’t specify exactly how many subjects are in these “relatively small” trials. However, the 2011 edition stated that “relatively small” meant that such trials are “usually limited to a few thousand subjects.”
The rate of disability or death among healthy children from any of those three diseases is incredibly rare. PIC wrote:
“For children under age 10 at normal risk (i.e., with normal levels of vitamin A and infected after birth), the pre-vaccine annual risk of death or permanent disability from measles, mumps, and rubella respectively was 1 in 1 million, 1 in 1.6 million, and 1 in 2.1 million. …
“Therefore, the cumulative annual risk of a fatal or permanently disabling case of any of those diseases was about 1 in 500,000, and the risk over a 10-year span was 1 in 50,000.”
In other words, clinical trials would need at least 50,000 subjects to detect one case of death or disability from a measles, mumps or rubella infection.
Meanwhile, no safety studies on the MMR vaccine have been done that looked for possible genetic mutations, impaired fertility or cancer, according to the product’s package insert.
Dr. Liz Mumper, a pediatrician, praised PIC for releasing the collection of data on measles, mumps and rubella, and on the MMR vaccine.
“Most parents have not had access to the information contained in the thoughtful analysis done by Physicians for Informed Consent. Parents should recognize that the risk of bad outcomes from a measles infection — if their child lives in a developed country with clean water and is not immune-deficient — is extraordinarily rare, as PIC reports.”
Unfortunately, she added, recent U.S. media reports “sensationalized” the risks of measles.
What’s typically missing from measles media reports
Studies also suggested a link between a naturally acquired measles infection and a lower risk of asthma, eczema and hay fever.
Malnutrition — particularly vitamin A deficiency — is a primary cause of over 100,000 measles deaths in underdeveloped countries.
Mumper said that the risk of bad outcomes from a measles infection drastically declined with improved public health and better nutrition long before MMR vaccines were available.
“The risk of bad outcomes has always been more for children in developing countries who are more likely to have nutritional deficiencies including vitamin A and lack access to clean water,” Mumper added.
Last week, independent journalist Alex Berenson reported that a preschool-aged child died of “cardio-respiratory arrest” after taking a dose of Moderna’s Covid mRNA vaccine during its clinical trials. Despite federal requirements to report all trial information, the company withheld the truth for years as it raked in billions from its Covid shots.
The extent of the cover-up remains unknown, but Moderna, headed by CEO Stéphane Bancel, disregarded federal law requiring companies to report “summary results information, including adverse event information, for specified clinical trials of drug products” to clinicaltrials.gov. The company, not the government, is responsible for posting all results, and failure to report the death of a child constitutes a clear breach of US law, which threatens civil action against any party that “falsifies, conceals, or covers up by any trick, scheme, or device a material fact.”
To this point, pharmaceutical companies have remained largely immune for their role in perpetrating globally-scaled deception resulting in thousands of vaccine injuries and billions in profits. They have enjoyed a liability shield courtesy of the PREP Act, which offers protections for injuries resulting from vaccines; that indemnity, however, does not extend to non-compliance with federal regulations, material misstatements or omissions of fact, or other offenses.
The death of the child only became known because of an obscure European report released last year, which revealed that Moderna has known about the death for over two years while it continues to advertise Covid shots to children as young as six months old.
Moderna’s European filing also revealed that the company withheld trial results demonstrating that children under 12 who received the vaccine were ten times more likely than those who received the placebo to suffer “serious side effects.” Without any evidence, Moderna claimed that the side effects, including the death of a child, were unrelated to the shots.
The incoming Trump administration offers a rare opportunity to hold pharmaceutical companies accountable and to investigate the depth of the cover-up.
The FDA is responsible for enforcing the reporting of vaccine trial results, but recent heads of the agency such as Scott Gottlieb and Robert Califf have been fanatical supporters of Big Pharma. Trump’s choice for FDA, Dr. Marty Makary, presents a stark contrast to his predecessors. Makary has criticized the US Government’s reluctance to acknowledge the role of natural immunity in preventing Covid infection, and he opposed the widespread vaccination of children. He testified to Congress, “In the U.S. we gave thousands of healthy kids myocarditis for no good reason, they were already immune. This was avoidable.”
President-elect Trump has tapped Robert F. Kennedy, Jr., perhaps the most well-known critic of the Covid vaccines, to lead the Department of Health and Human Services, which oversees the FDA. He has named Dr. Jay Bhattacharya, an author of the Great Barrington Declaration, as his choice to head the National Institutes of Health. Further, Senator Ron Johnson (R-WI) told Berenson that he plans to subpoena the FDA once Republicans become the majority party in the Senate this month.
President Trump’s first term was ultimately defined by his failure to fulfill his pledge to “drain the swamp.” A corrupt bureaucracy, personified in many ways by Dr. Anthony Fauci, aided and abetted by advisors like his son-in-law, Jared Kushner, hijacked the president’s agenda. Now, the Trump administration has an unlikely yet monumental opportunity for health reform, which can start on January 20 with an investigation into Moderna’s cover-up.
The Covid response doomed Trump 1.0. Whether one regards this as a monumental error, the betrayal of a president by his advisors, an event beyond the president’s control, or a deeper and more complex plot involving everything and everyone associated with the government, both in the US and around the world, there is no question of the scale of the calamity for the public. The shots are part of that, the capstone failure of a long line of foreshadowing with lockdowns and all that was associated with pre-pharmaceutical interventions. The antidote came not as a cure but, for many, the disease itself.
Articles by Brownstone Institute, a nonprofit organization founded in May of 2021 in support of a society that minimizes the role of violence in public life.
As unprecedented rates of heart inflammation and damage emerge in the post-pandemic era, groundbreaking research reveals the heart’s remarkable ability to heal itself, supported by specific natural compounds.
The rising incidence of cardiac issues following widespread mRNA interventions has created an urgent need to understand and support the heart’s natural healing capabilities. While the full extent of injection-related heart damage continues to emerge, research showing the heart’s innate regenerative abilities – and natural compounds that enhance these processes – provides hope for those affected.
This research aligns perfectly with the groundbreaking work presented in Sayer Ji’s book “REGENERATE: Unlocking Your Body’s Radical Resilience through the New Biology.” The book explores how our bodies possess far greater self-healing capabilities than previously understood, including the heart’s remarkable regenerative potential. These insights are further expanded in the REGENERATE YOURSELF Masterclass, which offers detailed practical protocols for supporting the body’s natural healing processes.
The Heart’s Natural Healing Ability
Recent research has demonstrated that the heart contains resident stem cells capable of generating new heart muscle cells throughout life. This finding challenges the long-held belief that heart damage is permanent and irreversible. The discovery shows that the heart maintains a population of cardiac stem cells that can potentially regenerate damaged tissue under the right conditions.
Natural Compounds Supporting Heart Regeneration
Scientific research has identified several natural substances that show promise in supporting cardiac regeneration:
Resveratrol: Found in red wine and grapes, resveratrol has emerged as a powerful supporter of cardiac regeneration. Studies show it works by activating endogenous cardiac stem cells and improving myocardial regeneration following heart attacks. Research published in Molecular Medicine Reports demonstrates that resveratrol not only activates cardiac stem cells but also enhances their survival and function.
Geum Japonicum:This traditional herb has shown remarkable abilities to stimulate myocardial regeneration in animal studies. Research indicates it can support the regeneration of heart muscle tissue following damage, particularly in cases of acute myocardial infarction.
Rosa Laevigata (Chinese Rose): Studies have revealed that active compounds from this herb can induce substantial myocardial regeneration. The research, published in BMC Complementary and Alternative Medicine, shows it supports both regeneration and repair of damaged heart tissue.
Echinacea Combined with Wheat Germ: This combination has been shown to effectively mobilize stem cells that can home to cardiac tissue, potentially supporting natural regeneration processes. The research demonstrates their ability to enhance the body’s inherent regenerative capabilities.
Synergistic Approaches
What makes these findings particularly interesting is how these natural compounds work through multiple mechanisms:
Stem Cell Activation: Many of these compounds can activate and mobilize cardiac stem cells.
Anti-inflammatory Effects: They often provide complementary anti-inflammatory benefits that support the healing environment.
Antioxidant Protection: Several compounds offer antioxidant protection that helps preserve healthy heart tissue.
Cell Survival Support: These substances can enhance the survival of both existing heart cells and newly generated ones.
Practical Implications
This research opens new possibilities for integrative approaches to heart health. While conventional medical treatments remain essential for acute cardiac events, these natural compounds might offer supportive benefits for:
Recovery after heart damage
Ongoing cardiac health maintenance
Preventive heart health strategies
Support during conventional treatments
Understanding the Science
The research shows that these natural compounds work through various molecular pathways:
Exosome Stimulation: Some compounds enhance the production of exosomes, small vesicles that carry regenerative signals between cells.
Cellular Regeneration: They can activate specific genetic pathways that promote the formation of new heart muscle cells.
Anti-apoptotic Effects: Many of these substances help prevent programmed cell death while supporting healthy cell regeneration.
For more comprehensive research on this topic, interested readers can explore:
This emerging understanding of the heart’s regenerative capacity, combined with the identification of natural compounds that support this process, offers new hope for cardiac health – particularly relevant given current public health challenges. As unprecedented numbers of people seek support for cardiac health, these natural approaches, along with the comprehensive framework presented in “REGENERATE” and the Masterclass, provide valuable tools for supporting the heart’s inherent healing abilities.
The GMI Research Group (GMIRG) is dedicated to investigating the most important health and environmental issues of the day. Special emphasis will be placed on environmental health. Our focused and deep research will explore the many ways in which the present condition of the human body directly reflects the true state of the ambient environment.
Disclaimer: This article is not intended to provide medical advice, diagnosis or treatment. Views expressed here do not necessarily reflect those of GreenMedInfo or its staff.
Light therapy (photobiomodulation) shows promise as an effective noninvasive treatment for dry age-related macular degeneration, with 53% of patients gaining improved visual acuity over two years
The therapy uses specific wavelengths of light to enhance retinal cell function, protecting vision without injections or medications, and reduced new cases of geographic atrophy by 73%
Clinical trials demonstrated significant improvements, with treated patients averaging 5.4 letters gained in visual acuity compared to three letters in placebo groups, showing both safety and effectiveness
Photobiomodulation works by targeting mitochondria with red to near-infrared light (600 to 1,100 nanometers), increasing ATP production and reducing oxidative stress in retinal cells
While light therapy shows promise for AMD treatment, the best way to prevent this condition is avoiding seed oils, which contain linoleic acid
Light therapy, a painless, noninvasive treatment, could significantly lower your risk of vision loss from dry age-related macular degeneration (AMD), according to a study presented at AAO 2024, the annual meeting of the American Academy of Ophthalmology (AAO).1
Researchers revealed that photobiomodulation therapy, a type of light therapy, not only slows the progression of dry AMD but also improves visual acuity in patients. According to lead study author Dr. David S. Boyer, this therapy marks the first effective noninvasive treatment for dry AMD, offering hope to millions who have long struggled with limited options.2
Over two years, patients receiving this light therapy showed remarkable improvements: 53% gained more than five letters in visual acuity, and there was a 73% reduction in new geographic atrophy cases — signifying a significant decrease in the development of advanced damage to the retina — compared to those who didn’t receive the treatment.3 This therapy could soon become a standard, accessible option for preserving your vision without the need for injections or medications.
Understanding Macular Degeneration
AMD is a leading cause of vision loss, particularly affecting individuals over 50. The macula, a small part of your retina, is responsible for sharp, central vision — the clarity you need for reading, driving and recognizing faces. AMD exists in two primary forms: wet and dry.
Wet AMD is characterized by the growth of abnormal blood vessels beneath your retina, which leak fluid and cause rapid vision loss. This form is often managed with anti-vascular endothelial growth factor (anti-VEGF) medications.
In contrast, dry AMD progresses more slowly and involves the thinning and deterioration of your macula without the abnormal blood vessel growth seen in the wet form. Until now, treatment options for dry AMD have been limited to dietary supplements rich in antioxidants and lifestyle changes aimed at slowing the disease’s progression.
The Most Important Way to Prevent AMD
An ounce of prevention is worth a pound of cure, so before I go into the details of light therapy, I want to share the No. 1 way to prevent AMD — a disease process rooted in mitochondrial dysfunction and insulin resistance, triggered by the long-term consumption of seed oils rich in linoleic acid (LA).
Your eyes are highly susceptible to damage caused by polyunsaturated fats (PUFAs) such as LA.4 PUFAs are prone to oxidation, which means the fat breaks down into harmful metabolites, including oxidized LA metabolites (OXLAMs). These go on to cause mitochondrial dysfunction, which is a hallmark of most chronic disease.
Seed oils, including soybean, cottonseed, sunflower, rapeseed (canola), corn and safflower, are present in almost every processed food, including those from restaurants. To avoid it, you’ll need to eliminate most processed foods from your diet. Additionally, LA is hidden in seemingly “healthy” choices like chicken, pork and even olive oil, which is often blended with cheaper seed oils.
To protect your vision and overall health, it’s wise to keep your LA intake below 5 grams per day from all sources. If you can get it below 2 grams, that’s even better. To help you track your LA intake, make it a habit to enter all your foods into a nutrition tracker. That way, you can tally how much LA you’re consuming daily and adjust your meals accordingly.
Photobiomodulation (PBM) therapy uses specific wavelengths of light to enhance the function of cells in the retinal pigment epithelium (RPE), the layer of cells at the back of your eye that’s necessary for maintaining retinal health.
By improving cellular function, photobiomodulation keeps these cells healthy longer, slowing or even reversing the degenerative processes that lead to vision loss. Unlike conventional treatments, this therapy doesn’t require the discomfort and risks associated with injections or medications.
A study published in the journal Retina also revealed promising results of photobiomodulation therapy for dry AMD.5 This randomized, controlled trial enrolled 100 subjects across 10 U.S. centers. Participants were aged 50 and older, diagnosed with intermediate dry AMD and exhibited best-corrected visual acuity (BCVA) scores between 50 and 75 letters, corresponding to a Snellen equivalent of 20/32 (slightly below normal) to 20/100 (moderately impaired).
Participants were randomly assigned in a 2:1 ratio to receive either the multiwavelength PBM treatment or a placebo treatment. The PBM regimen involved nine treatment sessions over three to five weeks, repeated every four months for a total of six series over 24 months. The placebo treatment mimicked the PBM procedure but with significantly reduced light intensity.
Patients receiving PBM therapy experienced significant improvements. At the 13-month mark, those who received PBM experienced an average increase of 5.4 letters in BCVA, compared to a three-letter gain in the placebo group. This difference is statistically significant and clinically meaningful, especially considering the progressive nature of dry AMD.
Moreover, 55% of the PBM-treated eyes achieved a gain of five or more letters, and 26.4% saw an improvement of 10 or more letters. In contrast, only 40.8% and 15.1% of the placebo-treated eyes achieved these milestones, respectively.6
Stabilizing or even improving vision in early to intermediate stages of dry AMD significantly impacts daily activities and overall quality of life. Additionally, the PBM group showed fewer instances of visual decline, with fewer eyes losing five or more letters compared to the placebo group. These results underscore PBM’s ability to halt and even reverse some of the vision loss associated with dry AMD.
Safety and High Compliance Rates: A Promising Profile
The Retina study provided reassuring data regarding the safety profile of photobiomodulation. Throughout the 13-month period, only 22.3% of treated eyes experienced at least one ocular-specific adverse event, with the majority being mild to moderate in intensity.7 Importantly, no adverse event was reported by more than 5% of participants, and none led to discontinuation of the study.
Compliance rates were impressively high, with 88.2% of PBM-treated eyes fully adhering to the treatment protocol compared to 74.5% in the placebo group. This high level of compliance is indicative of the therapy’s tolerability and the minimal burden it places on patients, with each treatment session lasting less than five minutes per eye.
The favorable safety and compliance data suggest that PBM therapy is well-accepted by patients, making it a viable long-term option. The absence of significant phototoxicity or other severe side effects also positions PBM as a safe alternative to more invasive treatments currently available for AMD.
More Evidence Light Therapy Benefits Dry AMD
A separate study published in Ophthalmology and Therapy also provides compelling evidence on the safety and efficacy of photobiomodulation for treating dry age-related macular degeneration (dAMD).8 This randomized, controlled, double-blind trial involved 76 patients over the age of 50 with dAMD.
Participants were assigned to receive either the PBM treatment or a placebo procedure. The treatment regimen included two cycles of sessions spread over several weeks. At the four-month mark, patients treated with PBM showed a significant improvement in best-corrected visual acuity, with 20.3% achieving a gain of five or more letters compared to 8.9% in the placebo group.
Additionally, there was a notable reduction in drusen volume among the PBM-treated eyes, suggesting that PBM may help slow the accumulation of harmful deposits beneath the retina.
Drusen, yellow deposits under the retina, are a hallmark of AMD and contribute to disease progression. By reducing drusen volume, PBM therapy may help slow the advancement of AMD, delaying the onset of more severe stages like geographic atrophy (GA) or neovascular AMD (nAMD).
Importantly, the study reported minimal adverse events, with only mild ocular discomfort experienced by a fifth of the treated patients. The most common adverse events included mild symptoms like dryness and warmth at the application site, which were easily managed and did not lead to any discontinuations.
Exploring the Biochemical Foundations of Light Therapy
PBM therapy utilizes specific wavelengths of red to near-infrared light (600 to 1,100 nanometers) to target the mitochondria within your retinal cells.9 Mitochondria are the powerhouses of your cells, responsible for producing adenosine triphosphate (ATP), the primary energy source that fuels cellular functions.
When PBM light penetrates your retinal tissue, it’s absorbed by cytochrome c oxidase (CCO), an enzyme in the mitochondrial electron transport chain. This absorption enhances mitochondrial activity, leading to increased ATP production, which in turn boosts cellular metabolism and promotes the repair and regeneration of retinal cells.
Moreover, PBM therapy helps reduce oxidative stress by decreasing the levels of reactive oxygen species (ROS) and mitigating inflammation within the retinal environment.10 The benefits of light therapy also extend to other macular diseases, offering hope for broader vision preservation. One such condition is diabetic macular edema (DME), a complication of diabetes that causes swelling in the macula due to leaking blood vessels.11
Preliminary studies have explored PBM’s effectiveness in reducing retinal thickness and edema in DME patients. Additionally, PBM therapy is being investigated for pachychoroid disorders, a group of diseases characterized by an abnormal thickening of the choroid layer in the eye. Early studies suggest PBM could help reduce inflammation and enhance mitochondrial function in these conditions.12
Photobiomodulation, particularly low-level red-light therapy (LLRL), is also beneficial for myopia, commonly known as nearsightedness.13 A meta-analysis, published in Clinics and involving 685 patients with a mean age of 9.7 years, found that LLRL therapy was associated with better outcomes in two key measures of myopia progression: spherical equivalent refraction (SER) and axial length (AL) change.14
A comprehensive review of multiple studies also found that red light therapy, using wavelengths between 635 to 650 nm, effectively reduces axial elongation of the eye and slows the increase in myopic spherical equivalent refraction, suggesting the nearsightedness is progressing more slowly.15 What’s more, these benefits were observed in treatments ranging from just four weeks up to 24 months.
The Role of the Optical Window in Light Therapy
Understanding the concept of the optical window is fundamental to harnessing the full benefits of photobiomodulation therapy. The sun emits a broad spectrum of light, with over half (53%) falling within the red, near-infrared, mid-infrared and far-infrared wavelengths. These wavelengths are categorized into three main groups:
1. Ultraviolet (UVA, UVB, UVC) — Comprising 7% of the solar spectrum, these wavelengths are responsible for skin tanning.
2. Visible light — Spanning from violet to red (400 to 700 nanometers), visible light accounts for 39% of the spectrum and is essential for vision.
3. Infrared light — Making up the largest portion at 54%, infrared light ranges from 700 to 10,000 nanometers and is invisible to the naked eye.
The optical window, specifically between 600 to 1,100 nanometers, is where PBM therapy operates most effectively. This range, particularly around 800 to 810 nanometers, allows light to penetrate deeply into tissues without being significantly absorbed by hemoglobin, melanin or water.
Below 600 nanometers, light penetration is limited as it is readily absorbed by these pigments, reducing its therapeutic reach. By focusing on the optimal optical window, PBM therapy delivers targeted energy to your retinal cells, enhancing cellular function and promoting eye health without unnecessary absorption or scattering.
The Multifaceted Benefits of Near-Infrared Light
Near-infrared (NIR) light plays a pivotal role in the effectiveness of PBM therapy, offering several biochemical advantages that support retinal health. One of the primary benefits of NIR exposure is the significant increase in ATP production within your mitochondria. Enhanced ATP levels boost cellular metabolism, assisting in the repair and regeneration of retinal cells affected by dry age-related macular degeneration.
Additionally, NIR light stimulates the production of melatonin within your mitochondria. While 5% of melatonin is produced by your pineal gland, 95% is generated in your mitochondria and acts as a powerful antioxidant. This melatonin effectively reduces oxidative stress by neutralizing free radicals directly within your mitochondria, protecting them from damage and ensuring their optimal performance.
Furthermore, melatonin helps increase glutathione levels, a vital detoxification agent that eliminates toxins and reduces inflammation.
It also promotes the release of nitric oxide (NO), enhancing blood circulation and vasodilation. These combined effects make near-infrared light a cornerstone of PBM therapy, offering comprehensive support for maintaining and improving retinal health.
Tailoring Your PBM Therapy: Optimal Dosing Strategies
Achieving the best results with photobiomodulation therapy hinges on delivering the right dose of red and near-infrared light. The concept of dosing in PBM is akin to finding the “Goldilocks” zone — not too little to be ineffective, and not too much to cause inhibition. Scientific studies typically utilize doses ranging from 5 to 50 joules per session, where a joule measures the energy delivered in watts per second.
For general health benefits, a balanced approach is recommended. Aim for approximately 25 joules per session, which can be administered using a large PBM panel. This equates to about 10 minutes of exposure to the front of your body and another 10 minutes to the back, totaling 20 minutes per session. This dosage ensures sufficient energy penetration to stimulate cellular processes without overwhelming the tissues.
While natural sunlight provides some near-infrared exposure, many individuals do not spend enough time outdoors to reap these benefits consistently. PBM devices offer a more targeted and controlled way to deliver the necessary wavelengths for optimal health outcomes. For best results, consult with a health care provider experienced in PBM therapy to determine the most appropriate dosing regimen tailored to your unique needs and health goals.
Selecting the Right PBM Device for Maximum Benefits
Choosing the appropriate photobiomodulation device is essential to maximize the therapy’s effectiveness for your specific health needs. PBM devices vary primarily in the wavelengths they emit and their penetration depth. Red light is excellent for treating superficial skin conditions but doesn’t penetrate deeply into tissues.
On the other hand, near-infrared light penetrates much deeper, making it ideal for targeting muscle tissues, enhancing cognitive functions and supporting retinal health in conditions like dry age-related macular degeneration.
For comprehensive benefits, a mixed PBM device that emits both red and near-infrared light offers the best of both worlds. Such devices allow you to address both surface-level and deeper tissue issues simultaneously. However, achieving these combined benefits requires spending about 50% more time using the device compared to using a device that emits only near-infrared light.
When selecting a PBM device, consider factors such as the specific health condition you wish to treat, the required penetration depth and the convenience of incorporating the therapy into your daily routine. Devices with adjustable settings that allow you to customize wavelengths and dosages provide greater flexibility and efficacy.
Additionally, ensure that the device you choose is clinically validated and comes from a reputable manufacturer to guarantee safety and reliability. While avoiding seed oils to protect your vision and prevent AMD is highly recommended, the advancements in light therapy symbolize a significant leap forward in combating vision loss, offering renewed hope and tangible benefits for those affected by dry macular degeneration and other eye conditions.
Recently, new data emerged showing that the COVID vaccines persist for up to 700 days within patients (and likely longer). As this is quite concerning to many, I was required to write an article explaining how this happens, and how it relates to the egregious production process that characterized the COVID-19 vaccines.
Upsides and Downsides
A lot of things in life are trade-offs, and as I’ve gotten older, more and more I’ve come to appreciate how many things in our society boil down to the fact that the options for addressing them all have significant downsides, so in many cases no solution exists which is satisfactory to all parties involved.
As such, this dilemma is typically managed by some combination of the following:
• Having a biased focus which emphasizes the benefits of an approach a side supports and downplays its downsides (or conversely disproportionately focuses on the downsides of an opposing position). To this point, I’ve had countless issues I’ve debated both sides of and been able to effectively persuade audiences of each one—which highlights how subjective many of the entrenched beliefs we hold actually are (and, in turn, is why I put so much work here into fairly presenting both sides of each controversial topic I cover).
• Sweeping the downsides under the rug and gaslighting the populace into believing they don’t exist.
• Blitzing the public into supporting a questionable policy before they have time to recognize its downsides, and if that fails, overtly forcing them to go along with it.
Note: I believe one of the reasons why governments frequently do horrible things to their people is because they are put in the position of having to “solve” a problem (but with no truly satisfactory way to do it), so they become habituated to using the three previous strategies to push their chosen policies along and simultaneously develop a collective mentality that those questionable approaches are necessary for the “greater good.”
There are many different manifestations of this dilemma, many of which I believe are essentially reflective of a foundational concept in medicine—sensitivity and specificity.
An ideal diagnostic test would catch every instance of a disease (100% sensitivity) and simultaneously never have a false positive (100% specificity). Unfortunately, in almost all cases, this is impossible to do, and instead a trade-off exists where you can either prioritize sensitivity (which leads to a significant number of false positives) or prioritize specificity (which leads to a significant number of false negatives). During COVID for example, a decision was made to prioritize sensitivity with the PCR tests (by having a high replication cycle thresholds) so no cases of COVID would be missed, but this resulted in such poor specificity that the PCR tests effectively became worthless (except for drumming up fear) since they produced so many false positives.
As such, when tests are designed, attempts are made to ensure there is a good balance between sensitivity and specificity. In some cases this is successful (e.g., there are many lab results we will take at face value), but in many other cases, given the technology involved, it’s not really possible to do so (or it is, but lobbying led to overdiagnosis so a medical product could be sold).
Similarly:
• Many policies in the justice system aims to enact fall into this same situation. For example, an ideal death penalty is robust enough to deter murder (and keep violent criminals away from the public), but simultaneously lenient enough that it doesn’t accidentally execute innocent individuals. Since there is no way to have both perfect sensitivity and specificity on this, different states take radically different approaches to how they enforce the death penalty (lying all along the spectrum between sensitivity and specificity). Likewise, our judicial system was founded under the principle “innocent until proven guilty” whereas many other countries have judicial systems that are the exact opposite.
• In medicine, one of the greatest challenges is finding the appropriate dose, as people differ, so what might be a safe and therapeutic dose for one person could be toxic for another. As such, standardized doses are typically chosen by finding the best overall balance between efficacy (a sufficient dose) and safety (avoiding a toxic dose), but for many drugs, the standardized dose leads to many more sensitive patients becoming severely injured by the drugs (which is then commonly “addressed” by gaslighting those injured patients). Note: a much more detailed discussion on the art of dosing can be found here.
• Every medical intervention has its risks and benefits, and ideally, the job of a physician should be to accurately weigh those to determine the best treatment for a patient (while simultaneously conveying what they are to the patient). Unfortunately, in many cases, they don’t (which is a large part of why patients are so dissatisfied with the medical system).
Overall, there are three key takeaways from this paradigm I wish to focus on in this article:
1. It is often incredibly difficult to find an acceptable balance between sensitivity and specificity, and many of the conventions our society now follows were the result of years of debate and protest from both sides to find a palatable middle ground between the two.
2. In almost any sphere I frequently find rushed attempts to find an acceptable balance between two conflicting positions to be immensely flawed and prone to creating significant issues in the future.
3. Many of the issues with the vaccine program are encapsulated by this framework.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. To see how others have benefitted from this newsletter, click here!
How Vaccines “Work”
Note: many believe the immune system is one of the least understood parts of physiology, something I would argue is a result of immunological research being focused on making profitable pharmaceuticals (e.g., vaccines) rather than understanding how it works.
In the classical conception of immunity, there are two types, innate immunity and adaptive immunity, with the innate response being relatively nonspecific (so it can work against a wide variety of infectious threats, including those the body has never seen before) and the adaptive one, which is uniquely suited to eliminating the specific invading organism.
The most widely accepted explanation for how the adaptive immune system works is “clonal selection theory” which states that the immune system:
1. Uses a random generation process to create a vast pool of potential antigen matching sequences.
2. Has vast number of different immune cells that each have those sequences attached to them circulate the blood stream.
3. Waits for one of those immune cells to contact an invading pathogen that the sequence it carries matches.
4. Have each of the immune cells be programmed to start rapidly reproducing once they get a sequence match.
5. Through the previous 4 steps, make it possible to produce a large number of immune cells which are specific to an invading organism (because they can bind to their antigens and alert the rest of the immune system to the organism’s presence), and thus effectively neutralize the infection.
6. Once the process is complete, to leave behind memory B cells, which match the invading pathogen and are able to stimulate the immune response in a much more rapid fashion (thereby shortening the time that steps 3 and 4 take).
The theory behind vaccination is that if the specific immune response and memory B cells can be created before the body encounters a dangerous microbe, this can:
• Allow the body to mount a robust immune response before a harmful invading organism has time to multiply within the body and cause significant damage.
• Cause individuals to rapidly clear infections (rather than needing to wait for the adaptive response to kick in), thereby reducing or eliminating the amount of time they can spread the disease into the population.
• Cause individuals to develop an immune response at the site of infection (e.g., the membranes of the nose and throat), thereby preventing the organism from being able to colonize those areas and thus preventing its transmission.
Being able to do this is hence immensely appealing to governments, as it allows a single intervention (the vaccine) which can easily be distributed to everyone in a top-down manner (which is what governments are good at doing) to address a longstanding problem (infectious disease outbreaks) and more importantly, to allow the government to present the appearance of working in earnest to safeguard the public’s health. Because of this appeal, throughout history, governments will get deeply invested in vaccine programs, and then once issues arise with those programs, double-down on the vaccine (e.g., with mandates) rather than reconsider the wisdom of the vaccine program. Note: in a previous article, I showed how this misguided and tyrannical conduct has existed ever since the first vaccine (smallpox).
Vaccine Production
To “work” vaccines aim to mass produce a dangerous organism’s antigen without the organism itself being present and then administer that antigen into the body. By doing so, the intermediate stage of an infection (where the organism has already reproduced enough inside its host to have a large number of antigens be available to match a circulating immune cell) can be achieved without the individual being in danger of being damaged or overwhelmed by the infection.
Unfortunately, unlike chemicals which can be rapidly synthesized, antigens are complex enough that they can only be produced by biological systems. As such, to produce the antigen, one of the following is typically done.
• Mass produce the infectious organism, then “kill” it so that its antigens can be collected, but the organism itself is not able to cause infections.
• Genetically modify another organism to mass produce a desired antigen, then kill it and extract the antigen (e.g. the HPV vaccine does this with modified yeasts).
• Modify the live pathogen (typically a virus) so that it can still cause the infection and reproduce inside the recipient but simultaneously is “weakened” so that it is less likely to cause illness.
• Genetically modify a “benign” virus to contain the antigen but be unable to replicate in the human body, then mass produce it outside the body, and have the body develop an immune response to the virus and the antigen on it once it is injected.
• Introduce mRNA into cells so human cells can produce large amounts of the desired antigen, which the immune system then sees (e.g., on the surface of the cells) and develops an immune response to.
The basic problem is that none of these approaches are perfect, and each has both its ups and downsides. For example:
• Most can create autoimmunity.
• In those where only a single antigen is used (and the virus spreads from human to human), if the vaccine actually works, it rapidly stop working because the pathogen quickly evolves a new antigen that no longer matches the vaccine.
• It contrast, the multi-antigen ones (which don’t have that issue) are typically live attenuated vaccines, which then can cause those with weakened immune systems to develop infections from the vaccine itself (e.g., this happens with the polio vaccine—which is why the primary cause of polio now is from the vaccines rather than natural infections, but also can happen with others like the shingles and measles vaccine).
Furthermore, some infectious diseases respond fairly well to vaccination, but the majority do not, so at this point, the vaccine industry has already picked all the “low-hanging fruit” and hence faces an existential struggle to develop new proprietary (patentable) vaccines it can bring to market. For example, had it not been for COVID-19 (SARS-CoV-2), a SARS vaccine would have never been brought to market as it was well recognized the SARS virus was poorly suited for vaccination (which what we then saw throughout the pandemic).
Finally. even if a vaccine “works” it still has to be manufactured, and there are numerous cases of the tradeoffs being made resulting in a disaster. For example:
• To make the inactivated polio vaccine, the live polio virus had to be exposed to formaldehyde. However, the challenge with this was that if too much formaldehyde was used, it would damage the antigens on polio to the point they no longer matched those on the poliovirus, whereas if too little was used, some of the polioviruses would remain active and could then give the vaccine recipient polio. The creator of the vaccine (Salk) opted to prioritize efficacy over safety, which the government in turn supported, even when one of their own scientists (Bernice Eddy) warned them against releasing the vaccine (as it caused polio in her lab). That 1955 vaccine then infected at least 220,000 people with live polio virus in Cutter’s vaccine, of whom 70,000 developed muscle weakness, 164 were severely paralyzed, and 10 died.
Note: an identical issue had happened on a smaller scale (9000 infections, 12 severe cases, 6 deaths) in 1935 with an earlier version of the inactivated polio vaccine. Likewise, (as I showed here) there have been dozens of incidents where an insufficiently inactivated or attenuated diphtheria, rabies or yellow fever vaccines severely injured hundreds of people (as the attenuated vaccines faced a similar issue with it being easy to over or under attenuate).
• Growing viruses for vaccines requires having a cell culture to grow them in. Monkey kidney cells were chosen because they worked well for doing this, but unfortunately were contaminated with the cancer causing SV40 virus. In 1962, Eddy again warned the government about the vaccine, but they still chose to give it to the public (and retaliated against her for speaking out), which in turn led to a wave of cancer sweeping through America, which until the COVID-19 vaccines was unprecedented:
Note: many other viral vaccines (particularly the live ones) also have had harmful viral contaminants identified within them, but unlike SV40, that contamination has not been acknowledged. Most noteably, a strong case can be made that HIV emerged from virally contaminated vaccines (that had been grown in monkey tissues).
• After a potentially dangerous strain of influenza (due to it having similarities to the 1918 influenza) was identified, a rush began to make an emergency vaccine for it (despite the FDA’s chief influenza expert Morris accurately warning that strain posed no risk to America). Since it took a while to cultivate the virus for a live attenuated vaccine, in order to make the vaccine be produced fast enough to hit the market before the influenza strain disappeared, a decision was made to hybridize it with the PR8 strain, a fast growing influenza strain directly descended from the 1918 influenza. Morris warned against doing this, but was ignored (and fired). That 1976 vaccine subsequently injured a large number of people (including some of our patients) and was a publicity disaster for the US government.
• The anthrax vaccine used during (and after) the Gulf War required growing large amounts of the bacteria, killing them, and then filtering out the most toxic components from the final vaccine preparation. The issue the manufacturer ran into was that because of how dirty the vaccine was, its contaminants clogged the filters the manufacturer used, so “solve” the problem and be able to manufacture the vaccine at scale for the military, the manufacturer opted to use larger filters which did not clog, but also didn’t filter many of the toxic components out of the final products—which resulted in one of the most harmful vaccines in history being unleashed upon our military.
Pertussis vaccine is one of the more troublesome products to produce and assay. As an example of this, pertussis vaccine has one of the highest failure rates of all products submitted to the Bureau of Biologies for testing and release. Approximately 15-20 percent of all lots which pass the manufacturer’s tests fail to pass the Bureau’s tests.
Eventually, the injuries that vaccine created led to so many lawsuits that the manufactures could not afford to continue producing the vaccine, at which point, the 1986 Vaccine Injury Act was passed. This shielded the manufactures from all future liability from it (hence allowing them to stay in business), and eventually incentivized the production of a safer but more costly pertussis vaccine.
• Frequently when an antigen is produced, it cannot solicit a sufficient immune response (unless a lot of it is used—which frequently makes the vaccine too costly to produce). To solve this problem, cheap (and toxic) adjuvants which enhance the immune response to the antigen are used, thereby allowing an affordable amount of antigen to be required for the final product. When the HPV vaccine was developed, it was discovered that its antigen (along with standard adjuvants) could not mount a sufficient immune response to get FDA approval, so a decision was made to use an experimental (but much stronger adjuvant) which worked—but also gave a large number of recipients autoimmune disorders (at least 2.3%). Nonetheless, that trade-off was also accepted to get it to market.
In short, if you look at all these cases, a consistent pattern should be clear. Whenever there is a choice between getting a dangerous vaccine to market or holding off because there isn’t a way to do it safely, the vaccine industry will always do the risky approach (especially in “emergency” situations) as they know they can unconditionally rely upon the US government to promote the product as “safe and effective” and then legally shield them from the disaster which inevitably follows.
COVID-19 Vaccine Hurdles
When COVID-19 began, the industry faced three major issues:
• Whoever was the first to develop a successful vaccine would make a lot of money, but those whose products took longer to reach the market would like miss out on the bonanza.
• There was a finite amount of time the lockdowns could be sustained (which made people want to vaccinate so they could be “free”) and it was very likely the population would rapidly develop herd immunity to COVID-19—so they was a limited window to get a vaccine to market.
• It was extraordinarily difficult to make a safe and effective vaccine for SARS (e.g., decades of work had not yielded a viable product).
Fortunately for the industry, the WHO (and Bill Gates), in 2010, had enacted their “Decade of Vaccine” plan, and with the World Economic Forum (between 2014-2016) had developed a framework for pushing through emergency vaccines that could bypass the regulatory process in the event of a health “emergency.” This framework gave lavish lavish fiscal incentives for vaccine manufacturers and positioned unaccountable organizations like the WHO, Gates foundation, or the World Economic Forum as the directors of a future pandemic response.
Shortly after that framework was finished, the FDA on January 13, 2017 released extremely detailed regulations for obtaining emergency use authorizations, and five days later, Gates publicly announced his plan to the world. This framework was endorsed by pharmaceutical companies, including Pfizer Moderna and J&J, and when Operation Warp Speed was finally conducted in 2020, it mirrored the framework Gates had previously developed.
Note: Event 201, a Gates funded “simulation” exercise modeling the release of a dangerous SARS virus from China was conducted on October 18, 2019. Reading through it in December of 2019 allowed me to accurately predict how COVID-19 would play out. Likewise, on 9/4/2019, Gates invested 55 million in the company that produced Pfizer’s mRNA vaccine—which in two years was worth 550 million.
So as you might expect, the industry chose to adopt the fastest possible production pathway, and was quickly granted the legal immunity (and lavish funding) necessary to accomplish that.
mRNA Vaccine Challenges
Note: one of the major advantages to the mRNA platform was that its production turn around time was much faster than existing alternatives (e.g., growing a virus in chicken eggs). This was a key reason why Fauci’s agency made decades of investments to develop the platform (as with the existing options, seasonal flu vaccines had to start being produced long before the circulating strain was known—which frequently led to the annual flu vaccine being for the wrong strain).
For the mRNA vaccines to “work,” the following needed to occur:
1. An antigen needed to be chosen that was highly likely to elicit a robust immune response that suggested SARS-CoV-2 immunity (and hence could win approval).
2. mRNA matching that antigen needed to be produced at scale.
3. The mRNA needed to be able to get into cells.
4. Once it got into the cells, the mRNA needed to be produce sufficient protein to create an immune response.
Many who have examined Pfizer and Moderna’s vaccines were perplexed by the design that was chosen, as many of the immensely harmful decisions that were chosen strongly imply the vaccine was deliberately designed to harm as many people as possible. While this very well might be the case, many of those issues can instead be explained by the fact each of those 4 challenges was addressed in a way that prioritized getting a vaccine to market rather than producing a safe one.
For example, the spike protein was the most reactive (immunogenic) part of the virus and necessary for SARS to infect cells, so it was an ideal vaccine target. However, it was also a terrible antigen to chose as:
• The spike protein was highly toxic, so if it was mass produced within the body, it likely would injure the recipient.
• It was a rapidly mutating part of the virus, which guaranteed the circulating spike protein would quick evolve into a variant the vaccine did not work against it—leading to the remarkable situation where we mandated a vaccine for an extinct virus (which, in turn, caused those vaccinated to become more likely to catch COVID-19 as their immune systems were continually primed to respond to a different virus from that they were exposed to)—something best demonstrated by the Cleveland Clinic’s study of 51,011 people):
Similarly, when I was trying to understand the acute toxicity of the vaccines, I suspected the lipid nanoparticles used to produce the vaccines had to be responsible for their acute toxicity (e.g., which could be seen within seconds of it being put into blood) as those effects onset far faster than it seemed possible for significant numbers of spike proteins to be produced.
After I looked into, I realized that for decades it had been deemed impossible to produce mRNA carrying lipid nanoparticles that had sufficient safety and efficacy to produce viable vaccines (to the point pioneers in the technology like Robert Malone who had invested decades of work into it abandoned it as they felt it was impossible to make a lipid nanoparticle which were not cytotoxic). In turn, when I reviewed leaked Pfizer regulatory documents, I noticed that their lipid nanoparticle had been chosen on the basis of it being the only one that had efficacy—again suggesting safety wasn’t taken into consideration.
Note: there were many other safety issues with mRNA techonolgy (e.g., synthetic mRNA induced immune suppression and antigenic spike protein coating cells and causing the immune system to destroy those cells) that are beyond the scope of this article.
mRNA manufacturing
In my eyes, the two biggest production issues with the mRNA vaccines were producing them at scale and then having them produce spike protein in the body at scale.
Note: these were easy to predict as one of the greatest challenges the pharmaceutical industry, and particularly biotech faces is producing their products at scale—a process which typically takes years to work out, but for Operation Warp Speed needed to be done in a few months.
mRNA design
A major challenge with synthetic mRNA was that the immune system would rapidly break it down, which resulted in not enough of the spike protein being produced to trigger a sufficient immune response. This in turn was “solved” through pseudouridylation, a process where pseudouridine replaces uridine in mRNA molecules as pseudouridylated mRNA resists immune system degradation.
Unfortunately:
• This process occurs in a very limited and tightly regulated manner inside the body. At the time the mRNA vaccines were developed, there was limited understanding on the biological significance of pseudouridylation, however many (e.g., Robert Malone) felt the preliminary data showed this approach had serious risks (e.g., immune suppression).
• These existing technology for pseudouridylation causes it to occur in a random and haphazard way. As such, rather than being able to determine a “safe” dose of pseudouridylation, an all or nothing approach had to be adopted, which in turn led to a significant number of vaccines having “excessive” pseudouridylation (either due to how much of it happened to the mRNA or where in the mRNA the pseudouridylation occurred). In short, this approach was extremely reckless, and akin to playing Russian roulette but hoping everything worked out.
In turn, the pseudouridylation did “solve” the mRNA degradation problem (to the point it won an unscrupulous Noble Prize), but it also created a new issue—the mRNA (and spike protein production) persisting in the body for a prolonged period, and likely due to the haphazard nature of the vaccine’s production, it persisting much longer in some cases that others. Lastly, while this invention “won” the Noble Prize, there were also viable mRNA vaccines that did not utilize it (and hence did not have the risks it entailed).
Note: Codon optimization (which increases protein production from mRNA) may have also caused the vaccine to excessively produce spike protein in the cells.
mRNA preservation
One of the major issues with synthetic mRNA is that its immensely fragile, so even if it could be protected from immune degradation within the cells (e.g., via pseudouridylation) it still was highly susceptible to common environmental factors. As such, when the lots of finished vaccines were examined by regulators, they determined there was both significant degradation of the mRNA and significant variability in what mRNA was preserved.
This is one of the many tables from the leaked EMA documents (which shows how quickly mRNA is destroyed at normal temperatures).
As this degradation and the resulting “truncated mRNA” was one of the primary concerns from the drug regulators Pfizer “solved” this problem by having all of their vaccines be ultra frozen (under the belief this would prevent mRNA degradation). However, this was largely for show, and before long the practice was abandoned (e.g., many vaccine sites had vials sitting outside throughout the day).
Note: at the time I learned about it, I thought that the primary issues would be broken mRNA sequences producing unintended and potentially harmful protein sequences. We now believe it’s actually the opposite, and that this breakdown process was a blessing in disguise, as evidence gradually accumulated that the older vaccines were and the further from their production site they were injected into the body, the less toxic they were—suggesting that the vaccine’s toxicity was mitigated by portions of its mRNA breaking down and hence preventing it from producing as much spike protein.
Process 1 vs. Process 2
The original process used to produce the mRNA vaccine had two ways it could be done. In the cleaner process (which was used to produce the vaccines for the trials), mRNA was produced through controlled replications with minimal contaminants present. Unfortunately, this process could not be scaled.
As such, an alternative approach was done:
• E. coli bacteria were genetically modified to have DNA that contained the spike protein, antibiotic resistance, and the SV-40 promoter.
• Those bacteria were mass produced, then doused with an antibiotic (so those without the resistance gene and thus the spike protein gene) died and did not contaminate the final product.
• The remaining bacteria are killed and their DNA is extracted.
• An mRNA polymerase is used turn that bacterial DNA into vaccine mRNA.
• Everything besides the mRNA is eliminated.
• The mRNA is packaged into lipid nanoparticles.
The essential problem with this process was that it was not feasible to remove many of the contaminants from each stage of production and there was significant room for variability at each stage (and thus in the final product). While many contaminants could be an issue, the vaccine safety community primarily focused on the plasmids as:
• The SV40 promoter (a key part of the cancer causing SV40 virus) was grafted onto the plasmids as this was an effective way to increase mRNA production.
• If there was a genomic integration, it was likely creating indefinite spike protein production in the cells.
• When vaccine lots were analyzed for their plasmid levels, it was found the lots which more frequently injured their recipients had higher levels of DNA plasmids (suggesting either harmful genomic integration was occurring, that the plasmids were toxic absent genomic integration, or that they were a proxy for other harmful contaminants).
Inconsistent Manufacturing
Each of the previous points illustrates that the vaccine industry was not ready to bring the mRNA vaccines to market and that the manufacturing of them was rife with errors. Many other points also support this such as:
• Japan pulled 1.63M vials of Moderna’s vaccine after visible metal particles were found in them and when examining vaccine vials, Ryan Cole found glass shards in the vaccines. Both of these suggest the production of the vaccines was rushed to the point basic quality control steps were not taken.
We looked at all the different vaccines and I think one of the conclusions we came away with is that it’s just a hodgepodge..there were vaccines that seems as though there were no particles within them, almost nothing there it was almost like a saline shot and then there were Pfizer’s that were just packed with them and you just get the sense that the manufacturing of this is totally inconsistent…some were more concentrated and some were less.
Note: this suggests that there was either very poor mixing when the vaccines were packaged (leading to some having lots of the lipid nanoparticles and others none) or that the vaccine manufacturers were unable to produce enough vaccine to meet the existing orders and switched to packing placebo vials to meet their contracted orders.
• In one mass spectrometry examination of 4 vaccine vials, it was determined that the lipid nanoparticles, but not the mRNA, were present in each of the vials. This suggests that the vaccine was not prepared in a consistent manner, or that the manufacturers ran out of mRNA to fill the vaccines with.
• A large body of evidence from the adverse event reporting databases (compiled here) demonstrated that the toxicity of the vaccine lots greatly varied, which again was likely explained by inconsistencies in their manufacturing.
Note: in a previous article about the mRNA lipid nanoparticles, I showed how inconsistencies in the manufacturing of the vaccines likely explained why the vaccines tended to affect different organs in the body (as their charge was affected by how much mRNA they contained and the area they deposited in the body was influenced by their charge) and why some individuals had acute reactions to them.
Blot Gate
One method of analyzing which proteins are present is with an approach known as “Western Blot.” Periodically, individuals will fake Western Blots (which can be detected because its very easy to identify computer generated ones).
With the COVID-19 vaccines, Western Blots were meant to serve as a quality control measure which ensured the mRNA vaccine were producing their intended protein. However, when we examined the available Western Blots we discovered:
• Some of them were computer generated (and hence likely fake).
• Others showed proteins besides the intended vaccine antigen were there (possibly due to broken RNA fragments being turned into proteins).
All of this again suggested that there were serious manufacturing issues with the COVID vaccines, but a decision was made to sweep all of that under the rug to protect the vaccine manufacturers (particularly since the drug regulators willfully ignored this fraud).
Note: this is similar to how there was extensive fraud throughout the COVID-19 clinical trials to exaggerate vaccine efficacy and safety (which essentially invalidated all the data was gathered), yet even after the trial participants and trial supervisors repeatedly notified the FDA, nothing was done. Likewise, shortly before the vaccine rollout, Vanity Fair published an article highlighting the serious issues in Americas’s vaccine manufacturing plants and that the FDA essentially was unable to monitor them—hence arguing things would get even worse during Operation Warp Speed.
mRNA persistence
Once the COVID-19 vaccine hit the market and the injuries began to mount, we noticed a three curious patterns.
1. The susceptibility to vaccine injuries greatly differed, but in many cases seemed to cluster (e.g., I knew a husband and wife who got vaccinated at the same time and both have near fatal complications from the vaccine).
2. A significant number of individuals appeared to be sensitive to vaccine shedding, something that is supposed to be “impossible” but nonetheless was occurring in a fairly repeatable manner to a large number of people, with symptoms similar to COVID vaccine injuries but typically less severe. Note: everything we know about shedding is discussed here.
3. Many individuals with vaccine injuries appeared to be suffering toxic reactions to spike proteins in their blood steam months if not years after vaccination. For example:
• Autopsy studies (conducted on individuals who died suddenly up to 6 months after the vaccine) have shown that their tissues were flooded with spike protein. Beyond the inflammatory and necrotic responses to the spike protein being their likely cause of death, it also suggested those individuals had had large amounts of spike protein being perpetually produced within their bodies.
• Both myself and Pierre Kory have come across numerous cases of individuals with vaccine injuries who, months, if not years after vaccination, respond to spike protein binders (suggesting unbound spike protein was causing their issues). Additionally, those individuals either remained recovered, significantly regress, or partially regress once the binder is stopped (implying there is a sustained but possibly diminishing production of spike protein in the body in many vaccine injured patients).
• The only commercially available test for the spike protein (offered by Quest) measures existing antibodies to the spike protein receptor binding domain, and provides values anywhere from 0-25,000 (or higher than 25,000). Clinically, we’ve seen that long COVID rarely get levels above 4,000, whereas in those with vaccine injuries, it can be anywhere from 0-25,000 with many being over 25,000. In turn, a rough (but not precise) correlation exists between the antibody levels (which do not directly measure spike protein levels) and a patient’s illness (along with its levels improving or worsening generally correlating to a patient’s symptoms improving or worsening). Curiously, many patients do not have their antibody levels decline with time (which is what you typically see after a COVID infection), which again suggests spike protein is being produced within the body that then stimulates an immune response. Conversely however, some of these cases may instead have been from people who had antibody levels far above 25,000 who then had their antibody levels decline (but this cannot be detected as they are still above the 25,000 cut off). Note: Alex Bereneson has also shared reports of vaccinated individuals who’ve had spike protein antibody levels over 25,000 for months after vaccination.
Pivotal mRNA Studies
When the COVID vaccines were pitched to the public, two of the greatest concerns were that the experimental gene therapies could change our DNA and that they would persist in the body for a prolonged period. To address these sales barriers, the media continually platformed experts like Paul Offit and Anthony Fauci) who dismissed us by continually saying things like:
The vaccines cannot enter the nucleus of the cell
mRNA from the vaccines breaks down rapidly in the cell, so it does not have time to enter the nucleus and change your DNA.
mRNA is not DNA, so believing mRNA can change DNA represents a fundamental lack of knowledge of biology.
These points raised red flags to me, as beyond their being issues with each of them, no data was ever provided to disprove genomic integration of the vaccine (which would have been quite easy to do). As such, I assumed the vaccines did integrate into the genome, and evidence would eventually emerge that they did (and likewise that at least some of the vaccines would continually produce spike protein in the recipients).
Throughout this process, two very important, but largely forgotten studies came out.
Note: due to the extreme scientific embargo on anything which challenged the COVID narrative, it is somewhat of a miracle either of these were published.
The first was a March 2022 study from Stanford which showed that both vaccine mRNA and spike protein persisted at high levels at least 2 months after vaccination. This was highly unusual for mRNA, and suggested something (e.g., the pseudouridylation) was preventing it from breaking down. Most importantly, the study did not go beyond 8 weeks, so it was likely the mRNA was persisting for a much longer time.
The second was a January 2023 study (with many Harvard authors) which found in adolescents and young adults who developed myocarditis within a few days of vaccination, that compared to controls, they had significantly higher levels of free spike protein circulating in their blood (due to them not forming antibodies which bound it). This in turn suggested that those who were reacting the worst to the vaccines lacked the ability to form antibodies which could counteract its effects in the body, which both explained why some individuals were so sensitive to the vaccine (e.g., shedding) but also that those likely to “benefit” from vaccination also would have mounted a robust response against a natural infection (hence invalidating the justification for getting vaccinated).
Note: with the smallpox vaccines, vaccination was deemed successful if there was a strong inflammatory reaction at the vaccination site, whereas if no reaction occurred, the vaccination was deemed unsuccessful and the individual was repeatedly revaccinated (as when it didn’t “take” the individuals could still get smallpox). Many early medical dissidents observed that severe reactions to the smallpox vaccine typically followed the vaccine not “taking.” They hence came to believe that the smallpox vaccine working was due to the recipient having a functional immune system that could both already fight off smallpox and create the superficial inflammatory reaction to the vaccine and that the vaccine was simply taking credit for what their immune system could already do. This study made me wonder if something similar has occurred with the COVID-19 vaccines.
Most recently, Yale’s immunology team (which had previously strongly endorsed using the vaccine to prevent COVID and to treat long COVID—which is often disastrous) conducted a longterm study of the effects of vaccination on immune function. Recently, they shared their preliminary results with the participants and disclosed that they were having difficultly publishing the study due to the political pushback they were receiving.
Note: it is extremely common for studies which challenge a medical dogma to never be published. For example, the study demonstrating COVID vaccination causes shedding was stonewalled for well over a year, as I show here, many studies demonstrating harm from the childhood vaccines have been blocked from publication (or even being conducted), and in one well known incident, the CDC deleted data that incriminated the vaccine program. Likewise, I recently highlighted how once the ultrasound industry took off, research into its dangers abruptly ended (due to funding being withdrawn and journals refusing to publish it), which eventually created a collective amnesia that this data ever existed.
As the study was being conducted, a few of us were contacted by participants in the trial who kept us appraised of what was going on, but asked us not to disclose any of it so that we would not interfere with the trial’s publication (as Yale putting their name behind a study demonstrating longstanding immunological injury would make “long-vax” become a medically accepted condition—but the scientific community tends to react quite badly to study results being prematurely leaked).
Prior to that meeting, preliminary data had been published a 2023 pre-print (which has still not been published) which detailed the common symptoms seen in the 241 participants with post vaccination syndrome (PVS), which match what we’ve seen in clinical practice:
To quote the study:
In conclusion, people reporting PVS after covid-19 vaccination in this study are highly symptomatic, have poor health status, and have tried many treatment strategies without success. As PVS is associated with considerable suffering, there is an urgent need to understand its mechanism to provide prevention, diagnosis, and treatment strategies.
Note: these results were discussed in more detail in this October 2023 online conference (e.g., the mast cell component of the illness). From watching this conference, my impression was that the investigators sincerely want to help the trial participants, but due to the unpleasant implications of their findings, are in a very challenging position (hence why their 2023 pre-print has still not been published).
Recently, Alex Berenson decided to use his platform to publicize what was disclosed at the recent meeting, at which point, I felt it was appropriate to share some of what we’d learned, and shortly after it became a trending topic on 𝕏. There I highlighted that:
• There was a sustained drop in CD4 levels which the Yale group suspected could account for the sustained immune suppression following vaccination (e.g., AIDS is characterized by severe CD4 suppression). I do not know the average CD4 drop they saw, but one participant in the trial (who has extensive post vaccine symptoms) shared with me her labs which included:
• Study participants were found to have sustained vaccine spike protein in their blood (e.g., 700 days after vaccination), which led the researchers to suspect the vaccine was integrating into the genome.
Note: while there are no commercially available spike protein tests (instead we have to test the antibody levels), research institutions like Yale (and the studies I cited above) have access to tests for free spike protein. Fortunately, after years of work, a commercially available (and affordable) blood spike protein test appears to be just around the corner.
All of this briefly means:
• There is objective proof that long vax is a real syndrome. Unfortunately, given the pace at which science works, it will likely be a few more years before it is formally acknowledged (which will likely dovetail with new pharmaceuticals to treat it entering the market and all remaining interest in the COVID vaccines disappearing). However, given that Trump promoted these vaccines (and has been unwilling to distance himself from them), I could see left-wing institutions like Yale accelerating their publication timeline so that this becomes widely publicized throughout his presidency.
• The persistence of spike protein in the body indicates that the 2022 Stanford study would have found positive results if it had tested patients more than two months post vaccination and that the spike protein antibody titers are indicative of spike protein persisting within the body.
Note: I recently discussed this topic with Dr. Malone (who I consider to be the most knowledgeable people in this area). We are both of the opinion that while genomic integration may play a role in spike protein persistence, the more probable explanation is simply that the body cannot break down the mRNA (and possibly the spike proteins) due to how it was modified. Presently, the data does not exist to quantify the scale of spike protein genomic integration, but with what is currently known (which could change as more data becomes available) cellular production of vaccine mRNA is most likely not responsible for the majority of the free spike protein found in the vaccine injured individuals.
Conclusion
Throughout my life, as I’ve come to feel that because of the bad trade-offs inherent to many policies or technologies, those behind them (particularly the government) will take an approach akin to trying to pound a square peg through a round hole (as government always defaults to utilizing the force at its disposal to solve the problems it encounters). In contrast, whenever I encounter situations where there really does not seem to be a good way to balance the trade-offs, I take that as a sign I need to consider a completely different approach rather than forcing the one I’ve committed to into working.
With COVID for example, I realized near the start that it would be an exercise in futility to address it with a vaccine—a truth much of the world has now had its eyes opened to. Instead, it was my assessment from the start that the best option would be to quickly develop viable treatments for the illness that could prevent severe complications from it and then allow infected individuals to recover with a strong immunity to the disease (and as we’ve now seen, natural immunity is vastly superior to vaccine immunity for COVID-19).
Unfortunately, rather than heed that approach, our medical apparatus decided to do everything it possibly could to push the vaccine upon us, while simultaneously doing all they could to bury the myriad of effective off-patent treatments developed for COVID-19.
Since the pathway Bill Gates put into place for lucrative accelerated approvals is still in place, I believe this highlights how important it is for us to actually understand how these technologies work and the trade-offs involved with them (which are never disclosed). In turn, it is my sincere belief that if the public had known part of what I presented here, they likely would have never taken the COVID vaccines. Similarly, as I’ve tried to illustrate here, contamination and poor production is a systemic problem with vaccines, and were robust independent testing to be conducted (so people actually knew what was in the vaccines they were taking), the demand for them would likely disappear until the industry was forced to clean up its act.
Overall, it is my belief that the most effective way to stop these unsafe products is to simply have enough people boycott them that they become financially unsustainable (and due to the new era of information diffusion we are walking into thanks to platforms like 𝕏, it’s actually possible). The FDA and CDC have lost an immense amount of trust because of how flagrantly they lied to the public, and have thus far refused to take any accountability for their actions—something that will likely change once financial pressures (e.g., people no longer buying the drugs rubber-stamped by the FDA) force the agency to make genuine amends for its conduct throughout the pandemic.
While COVID-19 was a profound tragedy, because of it we now have an extraordinary opportunity to fix this continually proliferating corruption, and I sincerely thank each of you who has helped to make this moment possible.
An updated index of all the articles published in the Forgotten Side of Medicine (including the DMSO ones) can be viewed here. Additionally, to learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here.
Have you ever felt your money was wasted on supplements? That even though you consistently followed the protocol from your health-care practitioner you were not getting the results others obtained with the same program? You may have been right! We’ve helped hundreds of patients with age-related macular degeneration (ARMD) with these healing secrets designed to help “non-responders”; those for whom the average supplement and dietary protocol fails to work.
ARMD is the leading cause of blindness in elderly Western populations and it is marked by central vision loss where blind spots or scotomas intrude. Threading a needle and passing the driver’s licensing test eventually become impossible but ARMD is preventable – even reversible to some degree with the diligent, intelligently targeted efforts we have put into practice in our clinics to increase the chances of success.
The best doctor’s recommendations or nutritional consulting for ARMD are fruitless unless nutrients are able to be broken down or micellized, transported to the macula, and assimilated there. After years of observing how some patients prevent ARMD despite strong hereditary tendencies, how some halt or even reverse impending blindness, and how some patients actually get worse despite being on the same protocol, it became clear that powerful tactics were needed in addition to recommending dietary changes or supplements.
The strategies we employ are successful for many individuals and have applications far beyond the diagnosis of ARMD. They will influence conditions or diseases where proper fat breakdown is essential to impact issues such as dry eye, post-cholecystectomy (gallbladder surgery) status, liver disease, etc. The eye, GI tract, liver, and gallbladder are intricately entwined. Think about it, when your liver is sick, your eyes turn yellow or jaundiced. When your GI tract is out of balance, red, itching “allergy” eyes often result. Interesting signaling! The solution is more complicated than just popping a supplement or even making some dietary changes. Are you ready to learn the secrets? Whether you have macular degeneration or not, these concepts will serve you well.
Best Kept Secret #1: Work from the GI Tract Outward
Some doctors, when pressed if they had only one system to specialize in, would tell you, “The GI tract.” Why? Because the GI tract is central to good health and its ability to affect the entire body so powerful when operating at its peak. It is here that we begin to improve vision. The target nutrients used in past studies[1] to prevent, halt, or reverse ARMD are lutein, zeaxanthin, beta-carotene, antioxidants, and fish oil. The carotenoids (lutein, zeaxanthin, and beta-carotene) concentrate in the central part of the retina, and help us identify colors and see fine details, so they are vital in a healing strategy. They also provide protection against blue light, which damages the retina. Building macular optical pigment density (MOPD) is the goal in this approach, replenishing the macula; but first we have to break down these carotenoids and antioxidants and then shuttle them to the macula by following several simple tactics.
Dr. Stuart Richer, who demonstrated success in reversing macular degeneration with the LAST studies,[2] shares an encouraging increase in MOPD in the pictures below. From July 14, 2011, to October 6, 2011, the degree of MOPD increased by employing some of the following strategies. A picture is worth a thousand words and is the tool best used to motivate patients to committed action. These pictures give hope to those losing their eyesight; the macula is refilling nicely with lutein and zeaxanthin.
The graphs show MOPD, at baseline on the left and increasing in the right-hand picture reflected by the non-red portions of the image after nearly three months of supplementation use. This means the macula is refilling with luteinand zeaxanthin.
To ensure proper breakdown of supplements, use a good digestive supplement, preferably one that contains ox bile, taurine, lecithin, and adequate hydrochloric acid, or a combination of these. Thinning the bile is a major key to eye health as it will help more lutein get to the macula. Doing a liver/gallbladder flush[3]seasonally is an aggressive part of the plan, if one wishes to take a serious, logical approach. Remember, the liver and gallbladder influence the eye, so aim to create a healthy, fully functioning liver and gallbladder. We are not only our eyes. We are a complete system, so thinking from a systems biology approach[4] may create the desired healing response. To do this, head south to the GI tract first.
Interior Terrain Influences Absorption, So Start Clean
A well-functioning GI tract influences the eye tremendously. Support digestive ability by following the 4-R[5] or GI Restoration program. Absorption of the macula-replenishing carotenoids like beta-carotene will be hindered by the presence of Helicobacter pylori bacteria and/or an imbalance of intestinal bacteria. This interior terrain needs a healthy balance of good bacteria versus bad bacteria by using targeted supplements and the support of digestive enzymes along with the other approaches discussed in the 4-R protocol.
All of the targeted supplements and carotenoid-rich foods we suggest will not do you a bit of good unless they are first broken down or micellized.
As even Wikipedia notes, “Micelle formation is essential for the absorption of fat-soluble vitamins and complicated lipids within the human body. Bile salts formed in the liver and secreted by the gall bladder allow micelles of fatty acids to form. This allows the absorption of complicated lipids (e.g., lecithin) and lipid soluble vitamins (A, D, E and K) within the micelle by the small intestine.”[6]
These are the micellizing “magicians” that get the job done: (1) Ox Bile: Supply exogenous ox bile, particularly to post-cholecystectomy patients; (2) Lecithin: (Sunflower or soy) can be added to the diet to aid in fat breakdown; and (3) Taurine: A precursor to bile production, which also thins bile.
Fat-soluble lutein and zeaxanthin, essential to replenish the macula, require being emulsified or broken down to the micellized state in order to enter the bloodstream for transport by a very surprising particle “shuttle,” high-density lipoprotein (HDL).
Sufficient, Well-functioning Bile Is Vital
Bile acids are made from cholesterol in the liver and stored and concentrated in the gallbladder where they act as an emulsifying agent to break up fat into smaller globules, making it more soluble or hydrophilic. This process is called micelle formation. Fat and fat-soluble vitamins like A, D, E, K, beta-carotene, and the carotenoid family are carried to the intestinal mucosa, absorbed into the lymphatic system, and then into the bloodstream. So what is the best kept secret? First, break down the fat-soluble vitamins and then get them to the macula by raising HDL levels to 61 or above. Do you know what your HDL level is?
We discovered this secret by observing hundreds of macular-degeneration patients and had noted in their history that many had had their gallbladder removed or else they were obese or otherwise compromised and had trouble digesting fats, as evidenced by their dry skin, dry eyes, weight gain, gas and bloating, or floating or shiny stools after fatty meals had been consumed. The connection was obvious! No gallbladder, fat maldigestion, or liver or GI issues equaled problems. Half a million people a year are opting for cholecystectomy (gallbladder surgery), not realizing that they can simply cleanse the liver and gallbladder with a “flush,”[7] which is basically an “oil change” that removes old, stasis bile and relieves symptoms in most cases. It is not hard or expensive to do and anyone can do it. And it is certainly worth a try.
However, we are concerned – particularly in a patient with macular degeneration who has undergone cholecystectomy – that fat-soluble vitamins be effectively broken down and absorbed. It is hoped that practitioners caring for macular-degeneration patients incorporate these strategies into their standard of care so that non-responders will have more chance of improvement.
But proper breakdown isn’t the end of the story. Nutrient transport is another key player. Call the HDL “Shuttle.”
Best Kept Secret #2: Lutein and Zeaxanthin Need HDL Particles
Lutein and zeaxanthin, critical components to replenish the macula, are carried in the bloodstream to the macula on HDL particles. That’s amazing. Carotenoids responsible for central vision hitch a ride on a cholesterol particle and hone in on their destination: the macula. And you thought cholesterol was the enemy … wrong! Cholesterol in a healthy ratio and thin bile are key players in this healthy-eye strategy.
Bile is made of bile salts, cholesterol esters, and lecithin. Keep cholesterol at a healthy, total level and at an optimal HDL-to-low density lipoprotein (LDL) ratio because if cholesterol is too low, we will not have enough of the raw materials we need to make bile. Be sure you have what it takes to make cholesterol. Even magnesium plays a part. Blood-serum concentration of lutein and zeaxanthin by proper breakdown of nutrients into micellized globules is important, but equally important is the ability to transport them to their targeted destination. Unless HDL cholesterol is adequate – at least 61 milligrams per deciliter – time and money are potentially wasted on supplements.
Strategies to Raise HDL
Since keeping your HDL at 61 mg/dl or over is important, you might consider the following strategies:
Exercise: Regular exercise that raises your heart rate for 20 to 30 minutes increases HDL.
Lose Weight and stop eating transfats: Carotenoids concentrate in the fat first, so if overweight, lose weight! Meantime, while you’re working on it, take more lutein and zeaxanthin and employ the most successful diet recorded to lose weight and reduce disease: the Hale Project[8] documented the amazing success of the Mediterranean Diet (MeDi). Not only is it a smart way to eat, but it also reduced all causes of death and disease by fifty percent in study participants aged 70-90 with active disease processes established after ten years adherence, practicing moderate red wine consumption, light exercise, and not smoking. Macular degeneration or not, this diet is proven!
Drink Red Wine or use Resveratrol: High-altitude or heat-stressed vine wines from Argentina, Chile, Australia, or damp, moldy vines found in areas like the Finger Lakes of New York are typically higher in resveratrol and will not only raise HDL but also influence health at 1-2 glasses per day. If you don’t drink wine or it is contraindicated for you, then use non-alcoholic resveratrol.
Take Niacin and Fish Oil: both increase HDL.
Quit Smoking: Besides reducing HDL smoking asphyxiates the eye.
Get an Oil Change: Remove all transfats from your diet and replace them with healthy, healing oils to raise your HDL. Employ olive oil, coconut oil, ghee, hemp oil, and flax oil.
There is strength in combining a multi-pronged approach, so consider employing the total approach. Preventing, halting, and even reversing blindness is worth every sacrifice or new habit employed to ensure success and these secrets are a winning combination.
Summarizing the Total Approach
Aim for an HDL of 61 mg/dl.
Lose weight, if needed, and take a combination of supplements proven to halt or reverse macular degeneration. If overweight, take more than the recommended amount of carotenoids or use water-soluble zeaxanthin. In either case, employ the MeDi. It extends life and reduces disease.
Take a supplement that supports proper fat breakdown along with a good eye vitamin.
Do the 4R program[9] and/or a liver/gallbladder flush in the Spring and Fall to improve fat assimilation.
Flush and nourish the liver/gallbladder.
Eat a preferably organic diet, rich in the carotenoids, to replenish the macular pigment (MOPD -remember the pictures?). Egg yolk, kale, spinach, collard and turnip greens lightly steamed, romaine lettuce, broccoli, Brussels sprouts, red and yellow vegetables, and fruits are all great sources.
*A special thanks to Dr. Stuart Richer, Dr. Donald Carroll, NTP, and Bill Sardi, Medical Researcher, for reviewing this article.
This article is for informational purposes only. By providing the information herein, I am not diagnosing, treating, curing, mitigating or preventing any type of disease or medical condition. Before beginning any type of natural, integrative, or conventional treatment or regime, it is advisable to seek the advice of a licensed healthcare professional.
Kat Carroll is Executive Director of the National Health Federation and Managing Editor of the National Health Federation’s magazine, Health Freedom News, and is on the Board of Directors of the National Health Federation Canada and the Advisory Board for GreenMedInfo. Kat received the NHF 2014 Health Freedom Hero award. She also writes for several publications, and is currently compiling a book on Codex Alimentarius based on first-hand experience attending International Codex meetings.
Kat maintains a private practice as a Nutritional Therapy Practitioner, certified in First Line Therapy, and is a member of the Nutritional Therapy Association and the Ocular Nutrition Society. Kat is also Clinic Administrator at her and her husband’s Optometry clinic, Medical Vision Center.
Additionally, Kat enjoys hosting guests at Adytum Sanctuary, their Pacific Northwest Retreat.
katacarroll@
Disclaimer: This article is not intended to provide medical advice, diagnosis or treatment. Views expressed here do not necessarily reflect those of GreenMedInfo or its staff.
An estimated 12.3 million Americans over 50 are affected by osteoporosis (“porous bone” or low bone density), and an additional 47 million younger Americans are in the early stages. Worldwide, the prevalence is 18.3%
Rates of hip fractures vary from tenfold to a hundredfold between countries, showing that low bone density is not a consequence of aging per se, but is dependent on lifestyle factors, including the use of certain drugs such as proton pump inhibitors (PPIs), the most popular heartburn medications on the market
PPIs are only recommended for short-term use, yet 60% of users report staying on the drug for more than one year; 31% are still on them after three years. More than 60% are also taking them to treat conditions for which these drugs are not indicated, such as indigestion
Dozens of studies show rates of hip fractures are elevated among both long- and short-term users of PPIs, and at all dose levels
More recent research suggests one of the primary ways by which PPIs damage bone may be by way of collagen, as these drugs have been shown to inhibit collagen production through several mechanisms of action
Americans spend a whopping $13 billion a year on over-the-counter (OTC) antacids (acid neutralizers) and OTC and prescription proton pump inhibitors (PPIs), which are the most popular heartburn medications on the market.1 It’s estimated that more than 15% of the population are on PPIs.2,3
Prescription PPIs like Nexium, Dexilant, Prilosec, Zegerid, Prevacid, Protonix, Aciphex and Vimovo inhibit acid production in your stomach and are routinely used to treat gastroesophageal reflux disease (GERD), a condition affecting about 20% of the U.S. population.4 OTC versions like Prilosec OTC, Zegerid OTC and Prevacid 24HR are also available.
Once prescribed, your doctor may keep you on a PPI drug for years, despite label warnings suggesting they be used only for short periods. One of the potential ramifications of long-term use of heartburn medication is osteoporosis. In the Nutrition Facts video above,5 Dr. Michael Greger reviews the evidence for this.
Your Osteoporosis Risk Is Highly Modifiable
As of 2020, an estimated 12.3 million Americans over 50 were affected by osteoporosis (“porous bone” or low bone density), and an additional 47 million younger Americans were in the early stages.6 Worldwide, the prevalence is 18.3%, according to data cited by Greger.
If your bones are getting compromised in your 40s or even 30s, your life expectancy, not to mention quality of life, will be seriously lowered. As noted by Greger, the good news is, osteoporosis is not an inevitable outcome even in advanced age, as lifestyle has been shown to play the greatest role in its development.
Rates of hip fractures vary from tenfold to a hundredfold between countries,7 showing that low bone density is not a consequence of aging per se, but is dependent on things like diet, exercise, alcohol use — and the use of certain drugs, including:8
PPIs and H2 blockers
Antidepressants, anti-anxiety and antipsychotic drugs
Antiparkinsonian drugs
Benzodiazepines and other sedatives
Systemic corticosteroids
PPIs Linked to Bone Fractures
The link between PPIs and brittle bone is strong enough that the U.S. Food and Drug Administration issued a safety alert on it in 2010, warning that the use of these drugs increases the risk of wrist, hip and spine fractures. As noted in that safety announcement:9
“The new safety information is based on FDA’s review of several epidemiological studies that reported an increased risk of fractures of the hip, wrist, and spine with proton pump inhibitor use.
Some studies found that those at greatest risk for these fractures received high doses of proton pump inhibitors or used them for one year or more. The majority of the studies evaluated individuals 50 years of age or older and the increased risk of fracture primarily was observed in this age group.
While the greatest increased risk for fractures in these studies involved people who had been taking prescription proton pump inhibitors for at least one year or who had been taking high doses of the prescription medications (not available over-the-counter), as a precaution, the ‘Drug Facts’ label on the OTC proton pump inhibitors (indicated for 14 days of continuous use) also is being revised to include information about this risk.
Healthcare professionals and users of proton pump inhibitors should be aware of the possible increased risk of fractures of the hip, wrist, and spine with the use of proton pump inhibitors, and weigh the known benefits against the potential risks when deciding to use them.”
However, in March 2011, the FDA removed the warning for PPIs sold over the counter, claiming they had “concluded that fracture risk with short-term low dose PPI use is unlikely.” The caveat, of course, is that users of OTC PPIs must then strictly follow usage recommendations to avoid the risk of bone fractures.
OTC PPIs are not to be used for more than 14 days in a row, up to three times in a single year. Chances are, many users do not stick to these parameters, and since there’s no warning label, they might not think anything of it.
According to one survey, 60% of PPI users stayed on the drug for more than one year, and 31% were still on them after three years. More than 60% were also taking them to treat conditions for which these drugs are not indicated, such as indigestion.10 So, overuse is clearly a problem.
What’s more, as noted by Greger, as of 2023 there are dozens of studies showing rates of hip fractures are elevated among both long- and short-term users, and at all dose levels. So, the FDA’s safety alert is seriously outdated.
PPIs and the Risk of Bone Fractures
Studies showing a clear link between PPI usage and bone fractures include a prospective study11 published in 2009, which found that use of the PPI omeprazole was “a significant and independent predictor of vertebral fractures,” with a 3.50 relative risk compared to nonusers.
Relative risk ratio refers to the probability of an event occurring in the exposed group versus the probability of the same event occurring in a nonexposed group.12 So, in this case, PPI users were 3.5 times, or 350%, more likely to fracture their spines during the six-year follow-up compared to those who did not use the drug.
A meta-analysis13 published in 2016, which looked at 18 studies involving a total of 244,109 fracture cases, concluded PPI use was associated with a “modestly” increased risk of all fractures, including hip and spine fractures.
Here, pooled analysis showed PPI use raised the relative risk of hip fracture by 1.26 times, and this was true both for short-term (less than one year) and long-term (more than one year) use. The relative risk of spine fracture was also 1.58 times higher, and any-site fractures 1.33 times higher among PPI users.
How PPIs Cause Osteoporosis
As for how PPIs cause osteoporosis, studies suggest they can affect bone density by:
Inducing hypochlorhydria (a state where production of hydrochloric acid production is absent or very low), which inhibits calcium absorption14
Dysregulating bone resorption, which is essential for healthy bone15
Secondary hyperparathyroidism caused by a negative calcium balance16
PPI-induced hypergastrinemia resulting in parathyroid hypertrophy or hyperplasia17
Gut microbiome alterations18
Hypomagnesemia (low magnesium)19
Interestingly, more recent research suggests one of the primary ways by which PPIs damage bone may actually be by way of collagen, as these drugs have been shown to:20
Inhibit Type 1 collagen found in bone by increasing the release of calcium and deoxypyridinoline (the latter of which provides structural stiffness to Type 1 collagen)
Inhibit the gene expression of several collagen types
Reduce total collagen levels by inhibiting expression of dimethylarginine dimethylaminohydrolase (DDAH)
Impair vitamin B12 absorption, which can lead to elevated homocysteine. High homocysteine increases the risk of fractures by altering the quality of collagen21
As noted in a 2020 paper in the Frontiers in Endocrinology:22
“PPIs may actually target the ECM [extracellular matrix] in general and members of the collagen family in particular to influence bone pathophysiology including increasing the risk of osteoporosis and osteoporotic fractures …”
Other Risks Associated With PPIs
Dependency is also a real risk. Research cited by Greger found that just two months of PPI therapy in healthy volunteers induced “acid-related symptoms” when the drug was withdrawn.23 Besides bone fractures, other health risks associated with PPIs include:24
Kidney disease25
Intestinal infections, including Clostridioides difficile infection — In one study, those taking PPIs had a 1.7 to 3.7 times increased risk of developing C. difficile or Campylobacter infection compared to nonusers26
Stomach cancer
Gastrointestinal polyps
Pneumonia
Heart disease27and heart attacks, even if you have no prior history of cardiovascular disease28
Erectile dysfunction
Premature death
Higher risk of knee replacement29
Dementia30and Alzheimer’s disease31,32— In one study, PPIs were found to cause statistically and clinically significant impairments in the participants’ executive functions, visual memory and planning function after just one week of use33
Natural Remedies for Treating Occasional Reflux Problems
If you use acid-blockers, you’re compromising your entire digestive system. You may also be compromising your bone health and significantly raising your risk of osteoporosis and serious bone fractures that take a long time to heal.
So, if you suffer from occasional heartburn, indigestion and other minor reflux symptoms, forgo the PPIs and try one or more of the following nondrug alternatives instead:34,35,36,37,38
Aloe juice — The juice of the aloe plant naturally helps reduce inflammation, which may ease symptoms of acid reflux. Drink about one-half cup of aloe juice before meals. To avoid its laxative effect, look for a brand in which the laxative component has been removed.
Apple cider vinegar (raw, unfiltered) — Take 1 tablespoon of raw unfiltered apple cider vinegar in a large glass of water before or directly after meals.
Astaxanthin — When compared to a placebo, this potent antioxidant was found to reduce symptoms of acid reflux, especially for individuals with pronounced H. pylori infection.39 The researchers concluded a daily dose of 40 mg of astaxanthin was effective for reflux reduction.
Baking soda — One-half to 1 teaspoon of baking soda (sodium bicarbonate) in an 8-ounce glass of water, or orange juice, will help neutralize your stomach acid and ease the burn of acid reflux. While I do not advise this as an ongoing remedy, it is effective on an “emergency” basis when you are in excruciating pain.
Ginger root —Ginger has a gastroprotective effect by suppressing H. pylori. It also accelerates gastric emptying which, when impaired, contributes to heartburn. Add two or three slices of fresh ginger root to 2 cups of hot water and let it steep for several minutes. Drink it about 20 minutes prior to your meal.
Sauerkraut — Consuming sauerkraut or cabbage juice will stimulate your body to produce stomach acid.
Glutamine — The amino acid glutamine has been shown to address gastrointestinal damage caused by H. pylori. Glutamine is found in many foods, including beef, chicken, dairy products, eggs, fish and selected fruits and vegetables. L-glutamine is widely available as a supplement.
Ripe papaya or a papain supplement — Papaya contains papain, an enzyme useful for breaking down both protein and carbohydrates.
Fresh pineapple or bromelain supplement — Bromelain is a proteolytic enzyme found in pineapple that helps digest proteins.
Pepsin supplement — Like bromelain, pepsin is a proteolytic enzyme involved in protein digestion.40
Betaine HCI supplement — Betaine HCl is the hydrochloride salt of betaine, not to be confused with betaine or trimethylglycine (TMG). As noted in a 2020 review paper:41 “… the most common recommendation for the use of betaine HCl supplements is usually implemented using an empirical test for low stomach acid whereby increasing doses of betaine HCl are given during sequential meals until such time as an uncomfortable sensation is noticed by the patient.
Along with improvements in symptoms of dyspepsia (or laboratory analysis of improved protein digestion), the lack of side effects acts is an empirical confirmation that low gastric acid production was contributing to poor digestion and/or dyspeptic symptoms.”
Bitters — Bitters have a long history of use in herbal medicinal traditions to promote digestion and/or to relieve digestive complaints.42
Slippery elm — Slippery elm coats and soothes your mouth, throat, stomach and intestines, and contains antioxidants that may help address inflammatory bowel conditions. Because it stimulates nerve endings in your gastrointestinal tract, it is useful for increasing mucus secretion, which has a protective effect against ulcers and excess acidity.
Vitamin D —Vitamin D is important for your gut health. Once your vitamin D levels are optimized, you will benefit from your body’s production of about 200 antimicrobial peptides that will help eradicate gut infections.
Zinc — Your stomach needs zinc to produce stomach acid, so make sure your body has the necessary raw ingredients. The recommended daily amount for adults is 8 to 11 mg. Zinc-rich foods include oysters, lobster, beef, cashew nuts, beans and raw yogurt. A zinc supplement can be used if you rarely eat these foods.43
Talk to Your Doctor About Getting Off PPIs
If you’re currently on a PPI, I strongly recommend working with your doctor to wean off it, as inhibiting stomach acid can raise your risk of other, far more serious health conditions, including:44
Osteoporosis
Asthma
Depression
Gallbladder disease
Migraines
Macular degeneration
Autoimmune conditions, including but not limited to Celiac disease, Type 1 juvenile diabetes, Grave’s disease (hyperthyroid), lupus, multiple sclerosis (MS), rheumatoid arthritis and ulcerative colitis
The best and safest way to do that is to work with your doctor to lower the dose you’re taking while simultaneously implementing the following lifestyle modifications:
Avoid reflux triggers and/or any food that irritates your stomach
Reseed your gut with beneficial bacteria from traditionally fermented foods or a high-quality probiotic supplement
Thoroughly chew each bite of food
Once you get down to the lowest dose of the PPI, you can start substituting with an over-the-counter H2 blocker like Pepcid (famotidine) which appears to be the safest of all the OTC H2 blocker options out there. Then, gradually wean off the H2 blocker over the next several weeks.
Reproduced from original article: https://www.naturalhealth365.com/improve-your-vision-and-bone-health-with-lutein-and-zeaxanthin.html
by: Patrick Tims, staff writer| April 24, 2023
(NaturalHealth365) Lutein, a type of carotenoid found in the macula, is often prescribed to reduce intraocular pressure in individuals with pre-glaucoma and glaucoma. However, a recent study published in JAMA Ophthalmology by the National Institutes of Health (NIH) shows that lutein is also helpful in decreasing age-related macular degeneration.
Additionally, when combined with another macular carotenoid called zeaxanthin, lutein can improve bone health, making it even more compelling to include these nutrients in your daily supplement routine.
Revolutionizing eye health: Uncover the power of lutein and zeaxanthin
In smokers, some “experts” suggest, the use of beta-carotene has been linked to an increased risk of lung cancer. However, two NIH-supported studies demonstrate that the use of lutein and zeaxanthin, as shown in the age-related eye disease studies (AREDS2), can effectively replace beta-carotene, leading to a reduction in age-related macular degeneration (AMD). This is significant as AMD is the primary cause of blindness among older adults in the U.S.
Over a decade-long analysis of the AREDS2 formula, zeaxanthin, and lutein were found to be effective replacements for beta-carotene. This formula not only reduces the risk of lung cancer caused by beta-carotene but also slows the progression of AMD. However, it should be noted that the participants in the study were already smokers. The primary goal of AREDS2 was to create a formula that could be utilized by everyone, regardless of smoking habits.
The results of the study demonstrate that this innovative formula is superior in slowing the progression of AMD and is also safer. The reduction or elimination of AMD is critical for maintaining good health, as this retinal degenerative disease can ultimately lead to blindness. While there is no conventional cure for AMD currently, treating it has the potential to reduce the rate of vision loss.
The dangers of beta-carotene for smokers: Why lutein and zeaxanthin are a safer bet
The initial AREDS study, conducted in 1996, demonstrated that a dietary supplement containing 15 mg of beta-carotene, 80 mg of zinc, 2 mg of copper, and vitamins C and E could slow the progression of AMD, specifically from moderate to late stages. However, subsequent studies revealed that smokers who took beta-carotene had a significantly higher risk of lung cancer than non-smokers.
In the subsequent AREDS2 study, the beta-carotene was replaced with 2 mg of zeaxanthin and 10 mg of lutein for individuals who had ceased smoking or never smoked. The study found that the use of lutein and zeaxanthin did not increase the risk of lung cancer and had the potential to reduce the progression of AMD by up to one-quarter. The study concluded with participants using the AREDS2 formula with zeaxanthin and lutein instead of beta-carotene.
A more recent study involving over 4,000 patients over five years since the previous AREDS2 study showed a 20% decrease in the risk of progression to late-stage AMD compared to those who took beta-carotene. It is evident that lutein and zeaxanthin are vital components in the fight for better eye health.
More benefits: Lutein and zeaxanthin support bone health
Recent studies have shown that zeaxanthin and lutein not only promote eye health but also strengthen bones, reducing the risk of osteoporosis in older adults. In a study involving participants aged 50 and above, it was found that the intake of these carotenoids can lead to stronger bones and reduced risk of fractures. However, it’s worth noting that a relatively high level of zeaxanthin and lutein intake was required to achieve these results.
Nonetheless, the dual benefits of zeaxanthin and lutein make them particularly valuable for vulnerable senior citizens. By incorporating these carotenoids into their daily supplement intake, older adults can enhance their vision and bone health and improve their overall health and longevity.
To learn more about how to properly supplement your diet, we suggest you work with an integrative health coach – who understands your entire health history and personal goals.
Written by Brenton Wight, Health Researcher, LeanMachine
Copyright [c] 1999-[y] Brenton Wight. All Rights Reserved.
This site is non-profit, existing only to help people improve health and immunity
Updated 26th June 2024
What is Macular?
AMD (Age-related Macular Degeneration) is a type of central vision loss.
Central vision is essential for driving, reading, facial recognition, etc. The macula is an area covering only 2.1% of the retina, and 5.5mm diameter, but the most important.
AMD is the leading cause of vision impairment in the over-40s in Australia.
If we look at the black dot in the grid above, one eye at a time, we should see perfectly straight lines and the black dot in the centre.
If we view the same grid but see any distortion in the chart, as this sample of advanced AMD vision, or if there is smudging or invisible areas, see an optometrist or ophthalmologist as soon as possible.
Types of AMD
1. Dry AMD (nonexudative AMD or atrophic AMD) is the most common.
2. Wet AMD (Neovascular AMD) affects only around 20% of sufferers, but is more serious.
Note: Often confused with Epiretinal membrane, often called a macular pucker, which can cause similar symptoms, but is quite different. This is a thin, almost transparent layer of fibrous cellular material, released from the retina and other parts of the eye into the vitreous gel that then settles to form a film over the macula, affecting vision. Epiretinal membranes can resolve on their own, and mild conditions may not need further attention. In some cases, Vitrectomy surgery may be required, involving removal and replacement of some or all of the vitreous humor (fluid or gel) from the eye, and lifting the film from the macula. Has a fairly good success rate.
Age-related is a misnomer
Doctors say the cause of AMD is unknown, but as it happens more in seniors, it is age-related, or genetic.
But the evidence now points to diet rather than age.
Dr. Chris Knobbe, Ophthalmologist and founder and president of the Cure AMD Foundation, believes that the skyrocketing rates of AMD worldwide are actually caused by the increased consumption of processed food, and has nothing to do with age or genetics.
Before 1925, there were about 50 reports of macular degeneration world-wide, even though Ophthalmologists had instuments to view the macula from the 1860’s.
Macular degeneration became only slightly more common in the 1940’s.
In 1975, over 4 million Americans had macular degeneration.
In 2019 there are over 180 million people with Macular Degeneration, and it is predicted that by 2040 this number will grow to over 280 million.
Research is now clearly pointing to processed foods as the culprit, mainly margarine, canola oil and other factory-produced franken-foods, already proven to cause cancer, cardiovascular disease, blood pressure, obesity, diabetes, stroke, and now AMD as well.
Preventing AMD
As there is no “cure” for AMD, prevention is our best option. Dietary changes can help prevent AMD, and at the same time, prevent cardiovascular, cancer, stroke, blood pressure, diabetes, obesity, Alzheimer’s and more.
Apart from the diet, we need to get more quality sleep, by eliminating blue light (computer screens) and sleeping in total darkness.
AMD Symptoms
AMD has no symptoms in the early stages.
Later symptoms include:
Distortion, but sometimes blur or missing image in central vision
Reduced definition of colours, or dim colour vision
Central vision blocked by dark shapes
Difficulty with close work, e.g. reading
Central vision loss
Macular degeneration does not cause any pain.
See an optometrist or ophthalmologist as soon as possible if you notice any symptoms, or have any distortion on the chart.
Depending on the type of AMD, there are treatments, diet and lifestyle changes that can slow or stop vision loss, and may even improve vision.
High risk groups:
Those over 60
Family history of AMD
Smoking = 3 x risk
Obesity
Those working with computer, phone or TV screens
Caucasians have a higher risk than other races
Those with high blood pressure
Diet containing trans fats
Cardiovascular disease
Females have higher risk
Smoking damages the retina, and increases risk of AMD an average of 3 fold. The retina requires a lot of oxygen, which is depleted in smokers.
Cause of AMD
Doctors still cannot pin-point a cause, but there are many things to help prevent or treat the condition.
Official AMD Treatment
Dry AMD Official medical treatments available for dry AMD appear to be very limited.
For now, positive changes to diet and lifestyle slows disease progression.
Note: Dry AMD can progress to wet AMD, so any sudden changes in vision should be immediately reported.
More info at: www.mdfoundation.com.au/content/dry-macular-degeneration-1 Wet AMD
The protein VEGF (Vascular Endothelial Growth Factor) is mainly responsible for leaking and growth of new blood vessels that result in rapid and severe vision loss, which if left untreated, becomes permanent.
Anti-VEGF drugs can be injected into the eye to slow or stop the AMD process.
Monthly injections are used for three months, then continued on an indefinite basis at an interval determined by the ophthalmologist in consultation with the patient. Injection treatment advice:
Injection treatment is not long, and normally carried out in the ophthalmologist’s rooms, but sometime in a day surgery facility.
Anaesthetics are given pre-injection, to reduce discomfort. If there is no apparent change in vision, appointments should still be kept to ensure there really is no change.
The Amsler grid should be used daily for each eye, any sudden vision changes should be reported urgently. Treatment may still require continuation, even if vision has stabilised or improved.
Read more: www.mdfoundation.com.au/content/wet-macular-degeneration
Stem Cell Technology
Scientists in Sweden innovated a method of treating blindness using embryonic stem cells to produce retinal cells. The team at Karolinska Institutet and St Erik Eye Hospital reported in March 2020, their approach of using CRISPR/Cas9 gene editing to amend retinal cell production so the generated cells can hide from the body’s immune system, protecting them from becoming rejected. Read more: www.news-medical.net/news/20200330/Developments-in-treating-blindness-using-retinal-cell-production.aspx
Promising FN3K (Fructosamine-3-kinase) Treatment
Ghent University researchers tested eyedrops containing the protein Fructosamine-3-kinase (FN3K), which was developed at VIB Ghent. FN3K is natural protein controlling glycation of proteins throughout the body. The researchers treated the eyes of mice with this protein and noted that the spots under the retina were completely absent in contrast with the shamtreated contralateral eyes. Also has promise for diabetes, COPD and many other conditions brought about by a bad diet of overheated foods causing Advanced Glycation End Products.
Always eat salads wherever possible, and for cooking, always use steaming, never frying or other methods that heat food over 120 degrees C.
Drugs for AMD
Lucentis® (Lampalizumab) is a drug that binds to Complement Factor D, a protein which is encoded by the CFD gene in humans.
It is a treatment for dry AMD, but appears to work best in patients with complement-risk genes. Genetic testing may be appropriate if this treatment is considered.
Eylea® (Aflibercept) is an anti-VEGF drug developed for wet AMD. Avastin® (Bevacizumab) is an anti-VEGF drug, originally developed as a cancer drug. Not registered by the TRGA (Therapeutic Goods Administration) for use in the eye, so this use is “off-label”. Typically used for Australians not eligible for the approved drugs Lucentis or Eylea via POBS (Pharmaceutical Benefits Scheme).
Laser Treatments
PDT (Photodynamic Therapy) combines Visudyne, a light-activated drug, with cool laser light, directed on the relevant retinal area to seal and halt or slow progression of abnormal retinal blood vessels. The patient MUST avoid sunlight for 24 to 48 hours after drug infusion.
Patients having PDT usually continue to lose vision in the first six months of treatment, but then usually stabilises, halting severe vision loss, where anti-VEGF drugs start working faster.
PDT is now rarely used for normal AMD, but sometimes used with an anti-VEGF drug for patients with the polypoidal choroidal vasculopathy type of AMD, as this condition does not settle completely using anti-VEGF drugs alone.
Laser photocoagulation uses a concentrated beam of high-energy thermal light, directed to the retina to destroy and seal leaky blood vessels. The laser also destroys the retina adjacent to the blood vessel, so is used mainly to treat a small percentage of wet AMD patients who have new vessels not in the central vision.
Laser photocoagulation has a 50% recurrence rate, so close follow up and monitoring is essential.
Natural treatment for AMD
Food is vital, but only natural food, nothing processed. Processed foods are anything found in a supermarket on a box, bag, can etc.
Natural foods are only found in the greengrocery section, preferably in the organic area.
We should all aim for all foods in this area, with at least one meal daily as raw food, because we must have enzymes for optimum health and immunity.
Enzymes in raw food are destroyed by heating to over 50 degrees C (122 degrees F) which is about the temperature of hot water at the kitchen sink in most homes.
When cooking food, steaming is best. If we heat food over 120 degrees C (148 defrees F) by baking in the oven or frying etc, then AGEs (Advanced Glycation End-products) are formed from proteins or fats, which, just like the AGE acronym, cause premature ageing, and a much higher risk for AMD as well as glaucoma, cataracts and other eye disease, as well as blood pressure, strokes, heart attacks, brain disease, diabetes and other “modern” disease that did not exist 100 years ago.
Best foods are green leafy vegetables, broccoli, brussels sprouts, cabbage, lettuce, capsicum, cucumber, lemons, bananas, apples, spinach and berries of all kinds.
Eggs are great, with Nature’s perfect packaging, but should be boiled for 10 minutes to destroy any pathogens, and not fried or any other high-temperature methods.
Limited full-fat dairy is fine unless there are allergies, but low-fat dairy should be avoided, as the nutrition is in the fat, not in the water.
Fish has Omega-3 fatty acids that benefit the eyes as well as the heart and brain. Again, steaming is the best way to cook fish. Coconut Oil was used in an animal study to show significant reduction in caspase-3 activity (a protease enzyme causing inflammation and apoptosis).
Coconut oil helped protect the integrity of healthy cells in retinas through an anti-apoptotic mechanism, supporting a direct link between caspase-3 and progression of light-induced retinal degeneration.
Coconut oil is one of the healthiest oils we can consume, also boosting brain function in a single dose, increasing HDL (“good” cholesterol), reducing body-mass index (BMI) and waist circumference. Coconut oil reduces wound-healing time when applied topically.
Supplements for AMD prevention
The AREDS (Age-Related Eye Disease Study) found benefits of high dose supplements that helped prevent or treat AMD, and recommended that those diagnosed with AMD or at high risk should use these supplements as a guide.
The original AREDS study of zinc and antioxidants slowed progression of AMD by 20% to 25% for those in the intermediate or late stage of AMD, and delayed vision loss. The follow-up AREDS2 study included lutein/zeaxanthin.
The AREDS2 formula (daily dose):
Zinc (as zinc oxide) 80mg
Vitamin C 500mg
Vitamin E 400IU
Copper (as cupric oxide) 2mg
Lutein 10mg
Zeaxanthin 2mg
However, LeanMachine regards most of these ingredients as sub-standard or even harmful, even though they helped those in the study.
One example of a product NOT to buy: Bausch & Lomb, PreserVision, AREDS 2 Formula claims to conform to AREDS2 formula, but LeanMachine does not endorse this product.
Their Vitamin E is a synthetic dl-alpha-tocopherol (natural versions have a “d” prefix, d-alpha-tocopherol, where a “dl” prefix means an artificial product), and does not contain tocotrienols or the beta, gamma and delta versions of each, which make up the 8 components of Vitamin E.
Also it contains titanium dioxide (brain and nerve damage and a Group 2B carcinogen)
Also contains food dyes red #40 and blue #1 (can be contaminated with cancer-causing agents).
Contains Cupric oxide, but negligible copper is absorbed from this form.
Zinc oxide is dangerous and can damage DNA.
While healthy foods will help delay AMD, as well as reducing risk of diabetes, cardiovascular disease, Alzheimers, obesity, other eye disease and more, there is often not enough healthy content available to give the AMD patient enough of the correct nutrition, due to intensive farming practices, combined with toxic chemical additives in the soil.
Lean Machine recommends a combination of a healthy diet, supplements and sun exposure for optimum nutrition.
Oxidative stress is a major factor in progression of AMD, so antioxidants are important.
Various vitamins and minerals have been proven to reduce AMD symptoms, but eye doctors seldom pass on this information.
Supplements do not make up for a bad diet. Supplements often only supply a single important extract, but whole, natural foods contain fibre, enzymes and many other important compounds, so LeanMachine recommends a combination of both.
The following are the main supplements LeanMachine recommends for AMD patients:
OptiZinc is much better absorbed and much safer than zinc oxide. Also includes copper, but not enough, see chelated copper below
Vitamin C
– Pure pharmaceutical grade ascorbic acid powder is economical and effective. 1/4 teaspoon daily is 1250mg, more than enough for AMD, and added benefit for preventing or slowing progression of cataracts
Vitamin E
contains the extra 4 tocotrienols missing from cheap vitamins. Also good for the heart
Chelated Copper is much better absorbed, and much safer than Cupric Oxide. Note: Metallic copper is bad for the body. Copper cookware should not be used, and a Reverse Osmosis system should be used for all drinking and cooking to help eliminate fluoride, metallic copper, lead, arsenic, aluminium and other toxins
Lutein with Zeaxanthin. Lutein is extremely important as an antioxidant for eye health. This product includes OptiLut which increases lutein bio-availability, and also includes zeaxanthin
LeanMachine also recommends the following as added protection for AMD:
Astaxanthin is an important antioxidant, 10 times stronger than zeaxanthin, lutein and beta-carotene, and 100 times stronger than vitamin E
Omega-3 supplements such as fish oil or krill oil can help prevent AMD, but not as helpful as two to three serves per week of real fish. Krill Oil is far more effective than fish oil, is sustainable and comes from the less-polluted Antarctic waters of the Southern Ocean.
Both contain EPA (Eicosapentaenoic Acid), DHA (Docosahexaenoic Acid) and Astaxanthin which benefit many other conditions as well
Bilberry is another antioxidant important for eye health. All berries are beneficial, but the extract is good where berries may not be tolerated in the diet
In addition, mitochondria health is essential. Foods improving mitochondria are:
1. Proteins such as fish, nuts, seeds, beans, lentils, eggs that support Glutathione and other amino acids which protect the mitochondria.
2. Antioxidants – colourful vegetables, fresh fruit, herbs, spices, berries. Best spices are cloves and turmeric.
Supplements for Glutathione include:
Inform the doctor of any other medical conditions and any other medications, vitamins or mineral supplements.
Other Eye Disease
Many other conditions affect sight, and I will discuss these later in separate articles. Of course, it is quite possible to have more than one condition, so early diagnosis is essential so we are more likely to be dealing with the first condition without confusing treatment with two or more conditions.
Here are a few of the most common:
Epiretinal membrane is often confused with Macular Degeneration, but is a film over the Macula
Diabetic Retinopathy affects blood vessels in the retina, and is the most common cause of vision loss among diabetics.
CMV Retinitis an infection of the retina, often affecting those with poor immunity or with AIDS
Diabetic Macular Oedema caused by fluid accumulation in the macula causing severe blurred vision
Retinal Detachment the retina separates from the nerve tissue and blood supply underneath it
Uveitis is inflammation of one or more of the uvea, the nerve tissue, and/or blood supply underneath. Common with Sarcoidosis
Eye Checkups
Everyone should get an annual eye check.
Most people are first checked by an optometrist, and when a problem is found they are normally referred to an ophthalmologist.
First, after a quick eye chart test, with and without glasses, amblyopia (“lazy eye”) is tested by covering one eye and looking for movement in the other eye, also ocular motility testing to determine how well the eyes follow a moving object, and stereopsis or depth perception.
Then a refraction test checks the degree of hyperopia (farsightedness), myopia (nearsightedness), astigmatism and presbyopia to determine a prescription of any eye-glasses required.
Eye drops are used to enlarge the pupils and allow better scrutiny of the inner eye. Warning:These drops can last 4 to 6 hours, and when the patient ventures out into bright light, the pupils cannot respond quickly by reducing the pupil size, so glare and blurred vision can make driving or other activities dangerous, but everyone has a different reaction, and sun glasses are a must.
The doctor uses a “slit lamp” and checks the eyelids, cornea, conjunctiva, iris, and lens. Conditions are checked for retinal detachment, dry eye, blocked tear ducts, drainage problems, cataracts, macular degeneration, corneal ulcers, diabetic retinopathy and other eye disease.
The retina is examined and usually retina photographs are taken for reference in future tests to check for any change.
Colour blindness is normally checked using the Ishihara Color Vision Test booklet, each page containing a circular pattern comprising many dots of various colors, brightness and sizes, making up a single digit number. The full test contains 38 fifferent pages, but a basic test will only involve 14 or 24 different pages. A colour-blind person will see no number, or a different number in this test. Any problems in colour blindness may indicate a health problem such as glaucoma, MS (multiple sclerosis), diabetic retinopathy, macular edema and other disorders, as well as color vision issues caused by long-term use of some prescription medications.
For colour-blind people, specially tinted glasses can improve the distinguishment and vividness of various colours as a vision aid.
The retina has cone photoreceptors, and the red and green cones are often most affected, causing “red-green colour blindness”.
Foods to avoid
Baked foods. Gluten from wheat products damages the gut, even if we are not diagnosed as a Celiac.
All baked goods are not natural, contain very little nutritional value, and have been subjected to high temperatures causing AGEs
Processed meats, as almost all cold meats contain sulfite or nitrite preservatives (chemical numbers in the 200 series) which are known to cause cancer and Alzheiner’s
Soft drinks, as almost all contain 211 or other 200 series chemical preservatives that cause cancer, as well as sugar and/or artificial sweeteners that also cause cancer
Fruit juices, as many have added sugar and/or preservatives, etc. Better to eat a piece of fruit, as the fibre aids gut bacteria and digestion, and the chewing slows down consumption. Immunity starts in the mouth, with saliva starting the breakdown of food. This benefit disappears when gulping down juice
Anything fried and almost everything else at the take-away counter. If we need take-away food, try a fresh apple and keep the doctor and the ophthalmologist away
Low-fat anything. Fat-reduced foods have been processed, and usually fats have been replaced with sugar, one of the worst culprits for inflammation and disease of all types
Any foods with added or “fortified” iodine, folic acid, iron, vitamin D, etc as invariably these are cheap supplements and are quite often causing damage to the body by blocking uptake of the real nutrients in food
Bad fats – Margarine – do not be fooled by unscrupulous advertising from margarine manufacturers who claim that margarine reduces cholesterol. Maybe it does at first, but cholesterol is not our enemy, only OXIDISED Very Low LDL is bad, and that is the main ingredient in margarine. Alternative: Coconut oil, butter, cold olive oil.
Canola oil – heat processing in production oxidises this fat. Cooking with canola oil oxidises the fat even more. NEVER use canola oil for anything.
Alternative: Coconut oil
Sunflower Oil – similar problem to canola oil. Flaxseed or coconut oil is a much healthier alternative.
Bad drugs
Paracetamol, panadol, acetaminophen, tylenol – different names for the same drug marketed as “safe and effective” but it destroys L-Glutathione, the body’s own master antioxidant, and damages the liver. Around 90% of patients on the liver transplant waiting list are there because of paracetamol overdose. Alternatives for pain:
(a) MSM – primarily for joint pain but helps reduce the sensation of any pain.
(b) Bacopa – primarily for slight blood thinning and higher brain function, but also helps with pain
Statins – cholesterol lowering drugs that increase risk of diabetes, clobber our Vitamin D, cause muscle pain, liver and kidney disease, reduced immunity, and on average may slightly reduce risk of a heart attack but increase death risk from all other causes, so most people taking statins will not live one day longer, and have a poor quality of life
Aspirin increases risk of Wet AMD by causing leakage of blood vessels under the macula, causing scar tissue.
Do not take aspirin for cardiovascular disease or pain, as the risks for internal bleeding and/or Wet AMD outweigh any advantages. Read more in my Blood Thinner article
Cooking Methods
The best cooking method is NONE. Heating food over around 50 degrees Celcius (about the temperature of hot water at the kitchen sink) destroys most or all of the beneficial enzymes, so salads, fruit or other cold foods should be consumed at least once daily. An organic apple a day keeps the doctor and the ophthalmologist away…
The second best cooking method is STEAMING, which means a maximum of 100 degrees Centigrade (212 degrees F). Other cooking methods heat food well over the safety limit of 120 degrees Centigrade. Over 120 degrees C, AGEs (Advanced Glycation End-products) form, which change the chemical structure of the food, causing damage to the mitochondria and many body systems.
Microwaving also damages the chemical structure of food, and studies show negative blood test results in humans after consuming microwaved food.
Treatments for wet macular degeneration
The following is part of a section from Mayo Clinic:
Wet macular degeneration treatments can help preserve existing vision and, sometimes, recover lost vision.
When facing a wet macular degeneration diagnosis, it can help to understand the main treatment options.
Medications to stop growth of abnormal blood vessels
When you have wet macular degeneration, your body sends chemical signals to generate new blood vessels that grow from under and into the macula.
These new vessels bleed easily and leak fluid, damaging the macula.
Certain medications called anti-VEGF drugs can block this growth signal and help stop new vessels from forming.
These drugs are considered the first line treatment for wet macular degeneration.
Medications used to treat wet macular degeneration include:
Bevacizumab (Avastin)
Ranibizumab (Lucentis)
Aflibercept (Eylea)
Faricimab-svoa (Vabysmo)
Your doctor injects these medications into the affected eye.
You may need injections every several weeks to maintain the beneficial effect of the medication.
In some instances, you may partially recover vision as the blood vessels shrink and the fluid under the retina is absorbed, allowing retinal cells to regain some function.
Some possible risks of eye injections include eye irritation, new floaters, increased eye pressure, inflammation, cataracts, bleeding and infection.
Some of these medications may increase the risk of stroke.
Using light to activate an injected medication (photodynamic therapy)
Photodynamic therapy is another treatment option for abnormal blood vessel growth in wet macular degeneration, however it is used less frequently than anti-VEGF injections.
In this procedure, your doctor injects a drug called verteporfin (Visudyne) into a vein in your arm, which travels to blood vessels in your eye. Your doctor shines a focused light from a special laser to the abnormal blood vessels in your eye. This activates the drug, causing the abnormal blood vessels to close, which stops the leakage.
Photodynamic therapy may improve your vision and reduce the rate of vision loss. You may need repeated treatments over time, as the treated blood vessels may reopen.
After photodynamic therapy, you’ll need to avoid direct sunlight and bright lights until the drug has cleared your body, which may take several days.
Treatment can help slow the progress of wet macular degeneration, and in some cases restore some vision.
In addition to discussing treatment options with your doctor, ask about low vision rehabilitation, which can provide you with strategies and technology to live a full life, even with reduced vision.
We use cookies to improve your experience on our site. By using our site, you consent to cookies.
This website uses cookies
Websites store cookies to enhance functionality and personalise your experience. You can manage your preferences, but blocking some cookies may impact site performance and services.
Essential cookies enable basic functions and are necessary for the proper function of the website.
Name
Description
Duration
Cookie Preferences
This cookie is used to store the user's cookie consent preferences.
30 days
These cookies are needed for adding comments on this website.
Name
Description
Duration
comment_author_email
Used to track the user across multiple sessions.
Session
comment_author_url
Used to track the user across multiple sessions.
Session
comment_author
Used to track the user across multiple sessions.
Session
These cookies are used for managing login functionality on this website.
Name
Description
Duration
wordpress_logged_in
Used to store logged-in users.
Persistent
wordpress_sec
Used to track the user across multiple sessions.
15 days
wordpress_test_cookie
Used to determine if cookies are enabled.
Session
Statistics cookies collect information anonymously. This information helps us understand how visitors use our website.
Google Analytics is a powerful tool that tracks and analyzes website traffic for informed marketing decisions.
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga
ID used to identify users
2 years
_gali
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
_ga_
ID used to identify users
2 years
_gid
ID used to identify users for 24 hours after last activity
24 hours
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
Clarity is a web analytics service that tracks and reports website traffic.






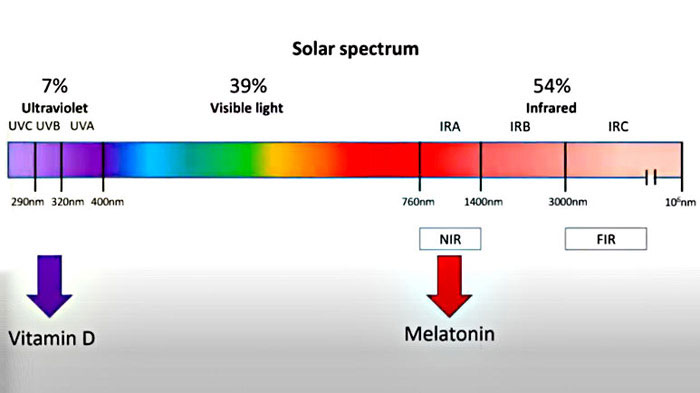





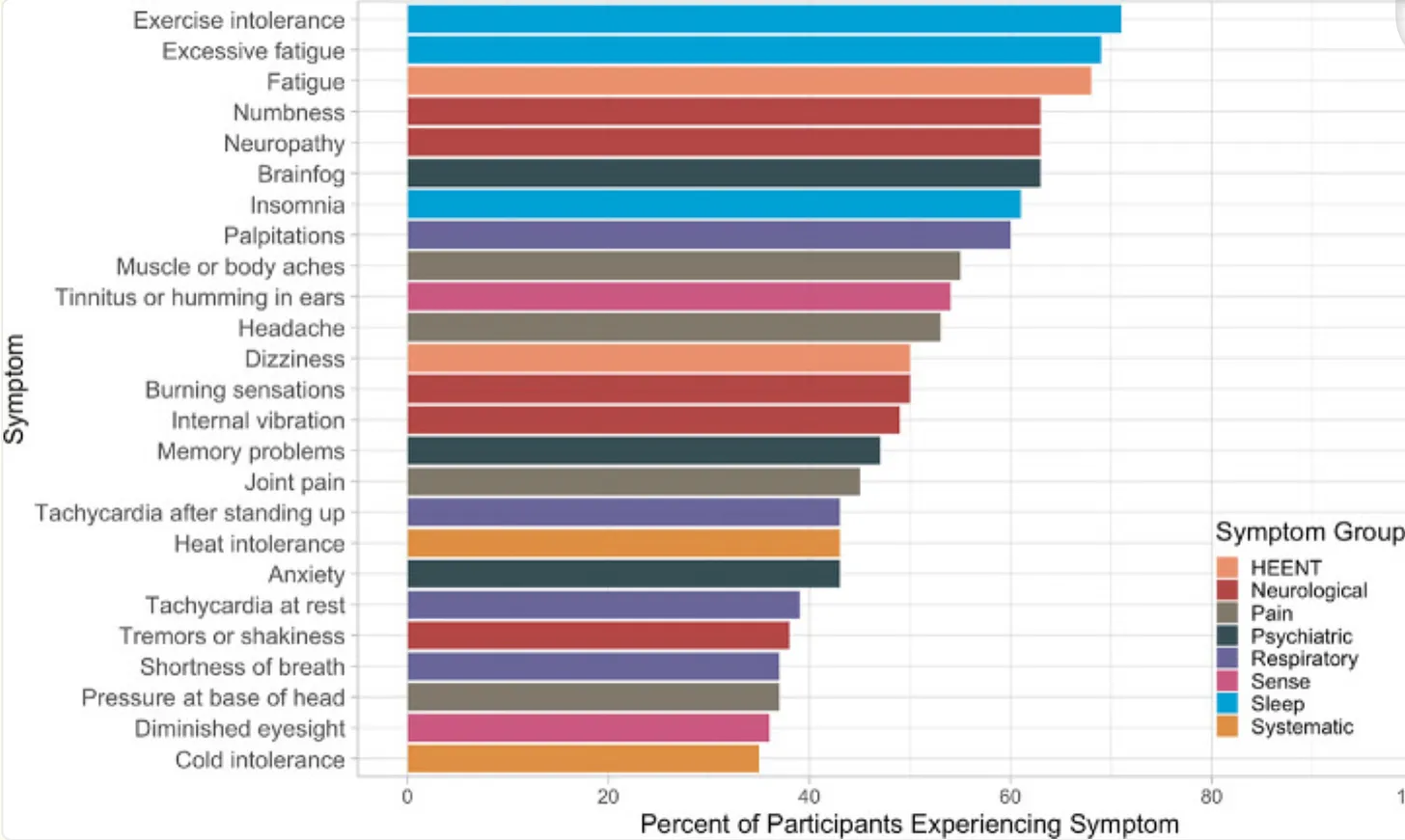






 Kat Carroll is Executive Director of the National Health Federation and Managing Editor of the National Health Federation’s magazine, Health Freedom News, and is on the Board of Directors of the National Health Federation Canada and the Advisory Board for GreenMedInfo. Kat received the NHF 2014 Health Freedom Hero award. She also writes for several publications, and is currently compiling a book on Codex Alimentarius based on first-hand experience attending International Codex meetings.
Kat Carroll is Executive Director of the National Health Federation and Managing Editor of the National Health Federation’s magazine, Health Freedom News, and is on the Board of Directors of the National Health Federation Canada and the Advisory Board for GreenMedInfo. Kat received the NHF 2014 Health Freedom Hero award. She also writes for several publications, and is currently compiling a book on Codex Alimentarius based on first-hand experience attending International Codex meetings. (
(




