In this interview, Dr. Suzanne Humphries discusses the release of the 10th anniversary edition of “Dissolving Illusions: Disease, Vaccines, and the Forgotten History,” one of my favorite books on vaccines, originally published in 2013. I was honored to write the foreword for the update of this classic.
In that book, Humphries details how vaccine science has been misrepresented to portray them as safe and effective, when in reality they’re neither. The vaccine industry has intentionally deceived us about the risks and benefits to make a profit, with complete disregard for the suffering they cause.
Questioning Vaccines Has Never Been Allowed
Humphries first became aware that vaccines might be problematic when she was working as a nephrologist in northern Maine.
“I was not a pediatrician, so I didn’t come at this from an autism standpoint or from an allergy standpoint,” she says. “I didn’t get to that until later. Early on, it was more about watching my patients who already had kidney failure experience worsening kidney failure after they were vaccinated or watching them bleed out after a biopsy of the kidney after they were vaccinated, because vaccines change your coagulation profile.
That was shown as early as the 1960s by an Italian researcher named Del Campo. He did one of the few studies that really tracked biological indicators and children over days, weeks and months, and found antacid production, inflammatory markers, coagulopathies.
In the end, he said vaccination is a trauma of considerable measure, and it should be undertaken with great caution. And yet, what we’ve seen since then is the addition of more and more vaccines to all of us, not just children …
I was basically watching adults have malignant hypertension, develop proteinuria protein in the urine, really nasty entities that are hard to deal with.”
After a three-year-long struggle with the hospital administration, who refused to listen to any of her concerns, she finally quit in 2011.
“That’s pretty much the history of me, being in the medical system, waking up, thinking that people around me would be interested in the medical literature that I looked at, which they never had looked at,” she says.
“Instead, I was ostracized and pretty much became a pariah. I just didn’t want to be there anymore. So, so I left. But the best decision I ever made was getting free of those golden handcuffs, where you leave medical school with this huge debt, and then you feel like you don’t have a lot of options after that. Pretty much every penny I earned went towards paying off my loans so that I could be free again.”
This is actually very common as the average medical school debt is about a quarter of a million dollars. Such a debt is indeed a pair of golden handcuffs that turn the physician into a debt slave, forcing them to work in positions with little to no autonomy when it comes to practicing the type of medicine they hoped they would when they applied to medical school. This is something I hope to address in the near future.
Dissolving Illusions
Shortly after quitting her job at the hospital, she wrote the first edition of “Dissolving Illusions” together with Roman Bystrianyk, who had been researching the history of disease and vaccines since 1998.
“What we decided to talk about was the history [of vaccines] because everywhere I went, talking about the flu shot that was damaging my kidney patients, I was met with, ‘Well, what about smallpox? And what about polio?’
And so, because I had to answer their questions, I learned a lot of things that I wouldn’t have otherwise learned.
Roman, who had gone through the world’s databases — he’s a computer guy, and he’s real smart — put these graphs and charts together [showing that] the death rate for many diseases was at least 96% decreased, sometimes 99% decreased, when vaccines and antibiotics came onto the scene. And so that was kind of the beginning of ‘Dissolving Illusions.’ We wrote the history around that.”
History Is Repeating Itself
According to Humphries, who has been “knee deep” in the vaccination issue for 16 years now, there’s a bigger picture that is only discernible when you look at the history of vaccines.
“What happens over time is, we’re able to sit back and look at everything that we have learned, and then re-weave it, and we see a bigger picture out of that … COVID, which, by the way, was probably no surprise to you and was no surprise to me … because if you do know your history, you know what’s going to come.
After the whole COVID debacle, and then reading about all the other vaccines, watching what happened with Gardasil, with the new flu vaccines, the old flu vaccines, and the childhood vaccination schedule just ever-growing, I sat back and I thought, ‘You know, this is just a repeating story.’
Vaccines, most of the time, if not all of the time, are marketed to the public as one thing, and then, later, the public discovers that they’re a different thing.
For instance, with COVID, the public was told it was just nice little particles of this virus put into saline, and it would stay in your arm. And then we have scientists that are now coming out — real bench scientists, real genetic scientists — who have broken down the constituents of the vaccine and are saying that there’s so much more in there than we were told.
Well, the same was true the smallpox vaccine. It didn’t have smallpox in it. Sometimes it had cow pox in it, sometimes it didn’t. Sometimes it had rabbit pus, sometimes it had the pus from horses, sometimes it had pus from goats and donkeys. And, and it was passaged back and forth between humans and animals because back then they thought that would strengthen the effectiveness of this so-called pure lymph, which was anything but pure.
So here, the public was told one thing, then doctors start crying out saying, ‘Wait a minute. This disease was not bad enough to cause this problem with the vaccines’ … Every vaccine that has come out, the public was told one thing, the effect is completely different. Doctors come out saying this isn’t what it was supposed to be, the doctors are ostracized, the doctors become afraid and don’t want to give reports.
This has been going on for 225 years. There’s been about 200 years of outcry from really upset doctors who were done in by the system for standing up for their patients and seeing the negative effects of vaccination.
So, we’ve added another 200 pages to our original book, ‘Dissolving Illusions,’ based on what we’ve discovered since. So, people who’ve already bought the book won’t be disappointed because there’ll be some new things included, and people who have never read it will get a bigger, deeper picture of the history.”
Critics’ Most-Oft Used Arguments to Dismiss Clinical Experience
Humphries initial foray into vaccine science centered around flu shots, because she wanted to know if they could cause all the kidney problems she was seeing, things like hematuria proteinuria, kidney failure, glomerular sclerosis or high blood pressure.
“I was just looking at that and wrote a 16-page white paper with 45 medical references and gave it to the CEO of the hospital, the head of nursing, my colleagues. I was met with absolute silence. I was really hurt and shocked by that, because it was a lot of work on my part. I really thought that people would be interested in it,” Humphries says.
“What’s interesting is that people want to nail us clinicians down to do the bench research, to talk about the genetics of a virus, to prove the existence of a virus, when what we’re watching in front of our eyes is a consistent repetitive timeline of somebody either marginally healthy or fully healthy, who gets a jab and then within hours, days or weeks develops horrible new medical problems.
This is what we see with the boots on the ground, but that’s considered irrelevant to people who want to discredit us. Our clinical experience means nothing. This is a way to just split us all into a million bits and say only the bench researchers can prove something. You can’t. So, you have to go do your own study.
That’s what was told to me. The Chief of Medicine of the hospital told me that he would support me if I wanted to do a research project on vaccine injuries in the hospital. To prove that you would need hundreds of patients, and he wasn’t really going to support me. He just wanted to divert me. That’s really what they want to do.
In terms of ‘do viruses exist or not,’ it’s the same thing. What we’re seeing is a consistent pattern. Children get measles one time in their life and don’t get it again. Children get chickenpox one time in their life, and then they don’t get it again. But because I haven’t personally viewed a virus under an electron microscope, my clinical experience means nothing.
So, this is how we’re dismantled and discredited by our critics. What I found is that if people don’t want to hear what I have to say, I just move on. I’m not going to get trapped in arguments with people, because there are so many individuals out there that know nothing.
I couldn’t care less about the brainwashed ignoramuses who are willfully ignorant. If they’re just innocently ignorant, then they’ll change pretty quickly. They’ll have questions and they’ll want to talk. But the people who are just like, ‘Well, what about this?’ … and won’t relent when the facts are piled up in front of them by somebody who’s done the work … Sorry, I have no respect for that.”
Vaccines Didn’t Eradicate Polio
So, just what happened with polio? As it turns out, polio was nearly eradicated well before the first polio vaccine became available. The primary reasons for its disappearance were the relatively rapid change in sanitation and hygiene.
“When I left my job, I spent about a year and a half pretty much doing nothing but researching polio from morning till night,” Humphries says. “I was given a library from the daughter of a very prominent physician in Illinois … He was the health department chair, and he waited to give the oral polio vaccine because he wanted to see what would happen, and because he had his doubts.
His name is Herbert Ratner. He collected a lot of information. So, I had a lot of public health reports to go through. I went through pretty much every book that was ever written about polio, both pro-vaccine and anti-vaccine and everything in between.
If you want to talk about gain-of-function and criminality, go ahead, and let’s talk about polio. Because poliomyelitis is a neurological entity, and it can be caused by a lot of different things.
So, in some ways, it was really brilliant for them to grab on to that pathophysiology and give it a name [after] a virus — a virus that’s actually a commensal [symbiotic] in the human body that’s been shown to cause no harm in most people …
Your immune system is always dealing with it, keeping it under control. But if you add a toxin to that, a toxin that increases permeability of the gastric mucosa, then all bets are off. Then, these entities can gain access.
The natural polio virus was not a thing that was necessarily being pathologically passed around to people. It was only when humans started tinkering around with it, like the gain-of-function experiment that happened at the Rockefeller labs in 1916.
During that exact time, there’s the world’s worst outbreak of polio with a 25% to 50% paralytic ratio. That was unheard of in 1916. So that would have set the stage for terror among the masses. We’ve got to get rid of this horrible disease. It’s crippling children, crippling adults. That’s when the movement to start developing the vaccine really began, and there were some horrifying failures along the way.”
The Failure of Salk’s Polio Vaccine Was Covered Up
As explained by Humphries, Jonas Salk was recruited to produce the first polio vaccine, and a massive propaganda campaign ensued to instill the idea that the polio vaccine was the greatest medical achievement there ever was. In 1954, Salk began a massive field trial of the vaccine that lasted one year. Millions of dollars were spent on it. It was one of the largest medical experiments in history, at the time.
At the end of the trial, there were scientists who disagreed with the design of the vaccine, and there were statisticians who spoke about its flaws. There were biochemist and biologists who warned the vaccine would cause a big problem, because if you don’t kill the virus, it’ll come back stronger. Alas, all detractors were replaced and the vaccine was licensed anyway.
Two years later, access to the complete database finally became available, and scientists who went through it “ripped it up, down and sideways,” Humphries says.
“It was absolutely a terrible design. The interpretations were incorrect. But by then the horse was already out of the barn. And isn’t that how it always happens? … So, that’s one side of the vaccine for polio.
The other side is that it was a very low-incidence disease. If you look at it on the charts in ‘Dissolving Illusions,’ we have all the diseases and the deaths. The incidence of polio, you can barely see it at the bottom.”
Change in Diagnostic Criteria Made Polio Vaccine Appear Effective
In the years that followed, most of the polio cases occurred in those who were vaccinated. In other words, the vaccine itself became a cause of polio. Natural polio was associated with paralysis, but most paralytic cases resolved within 60 days.
To make the vaccine appear effective, the diagnostic criteria for polio was changed. Initially, all you needed for a polio diagnosis was two physical exams, 24 hours apart. After the vaccine was released, the patient had to be reassessed after 60 days.
Since most cases resolved on their own in two months without intervention, this change made it seem as though the vaccine had remarkable effectiveness. Today, most polio cases worldwide are caused by vaccine-derived poliovirus (VDPV). So, VDPV has replaced natural polio infection.
Smallpox Vaccine Was a Major Killer
While the polio vaccine was rarely lethal, the smallpox vaccine turned out to be a major killer. According to Humphries, the death rate for smallpox infection was about 10 in 100,000. After the vaccine was brought out, the death rate for smallpox rose by 50%.
“That’s all documented from the UK. When they brought out the vaccine, the death rate from smallpox went up, cancer rates went up, tuberculosis rates went up. That’s what [smallpox vaccine creator Edward] Jenner’s subjects died from, they died from tuberculosis (consumption).
So, here we are today. We don’t have smallpox vaccines. The reason I think they got rid of it is because people were really analyzing and showing what was actually in it. And then we have scientists like Thomas Mac, who was still alive during the days of smallpox, saying that the vaccine didn’t get rid of smallpox. It was hygiene, it was cleanliness, and it’s not as easy to spread.”
Ever-Changing Goalposts
Another repeating story with vaccines is the changing of goalposts, such as the frequency at which you needed to get vaccinated, and how many doses you need to be fully protected. For polio, it went from one dose once in a lifetime, to four initial doses and a booster.
Why? Because the vaccine doesn’t offer lifetime protection. Few if any vaccines do, and that’s one of the primary differences between vaccine-induced immunity (which wanes) and natural immunity (which tends to be long-lasting, often for life).
“It’s the same story as the COVID vaccine,” Humphries says. “I’ve got patients now that have had five, six COVID jabs [and still got COVID]. When did it become okay to accept a vaccine and then still get the disease multiple times? …
Why on earth are we injecting ourselves with this putrid concoction with E. coli plasmids in it, when we could just use the technology that we have today, that good common sense that we have to support the divine blueprint instead of doing something diabolically against it, and injecting people numerous times with something that mis-programs their immune system so that when they are back in contact with it later, they’re going to have a worst time of it — original antigenic sin.
It’s been shown with flu, it’s been shown now with COVID. And it’s just a big mess. Seventy-five percent of my practice, for the first year, were vaccine injured people or people who had to go get the jab and didn’t feel they could get out of it and want it to be pretreated or post-treated.”
Humphries COVID Experience
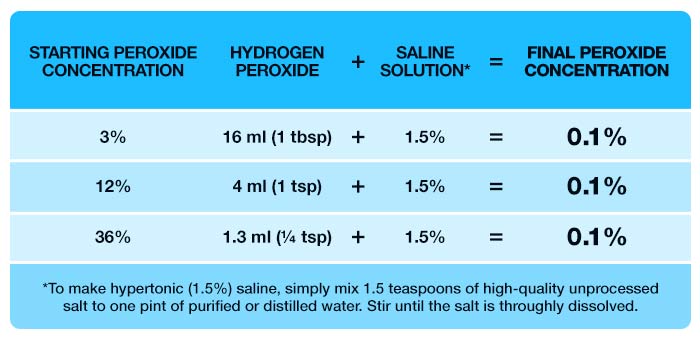
In the interview, Humphries recounts her own experience with COVID. She had a severe case that lasted two weeks. My go-to recommendation for any respiratory infection is nebulized peroxide. She used this, but still had a hard time overcoming the infection. In her case, one of the remedies that made the biggest difference was low-dose aspirin.
“For me, the thing that made me feel like I was not going to make it was the pain. I had total body pain. I don’t get headaches. I didn’t even really understand what headaches were until COVID came along and I just had the most horrible headache. So, for me, I believe in retrospect that it was the vascular aspect of it.
My blood wasn’t flowing properly, and the spike protein is really rough on the endothelium. The day that I took a quarter of a tablet of dissolvable aspirin, my whole world changed. My pain went away, and I felt like I was going to be OK.
So, I think for some of us, we just needed to get our blood flowing again properly. That for me was key, and I’m a big advocate of using very controlled low dose, as needed, aspirin when people are having the effects of COVID.”
I’m a big fan of low-dose aspirin as well. I take it every day. I think it’s a wise strategy for many. The reason aspirin has been vilified is because it’s a massive competitor to their high-priced NSAIDs.
Speaking Your Truth Can Change the World
Like Ashley Armstrong, who took a huge risk by leaving her engineering career to get into regenerative farming, Humphries can attest to the power of following your own truth and inner guidance. Sure, quitting her job at the hospital put her in a tough spot initially, but in the end, she’s better off for it — and so is the world. Over the past decade, her book has educated untold numbers of people about the truth behind the vaccine propaganda, and this update will continue to do so.
“When I left conventional medicine, I didn’t know how I would survive,” she says. “I didn’t have any debt, but I didn’t have any savings. It was friends and family that that helped me out. But when ‘Dissolving Illusions’ was published, we earned a little bit of money. Over the 10 years, it’s been what enabled me to not sink, and to not go into huge amounts of debt. It kept me afloat.
I just feel like God looks after us when we do the right thing. I feel like God has been 100% faithful to me, and that’s really what kept me going. I never imagined that in 2024, we’d be publishing another version of the book. But Roman brought that up to me about a year and a half ago.
I was like, ‘Oh, Roman, I’m so done with vaccines, I just want to have a life. I want to learn about the real physiology, how to really help people in front of me now. I want to start curing some of these diseases.’ That’s what I wanted to focus on. But he really wanted to do this, and I can’t say no to him …
I don’t know what holds for the future. Every year or two I like to bring a new project into my medical practice to learn a new thing and to offer a new thing. Sometimes the new thing ends up being a nothing-burger and I drop it, but I still like to explore, because we’re not at the end of the line in terms of what we can offer people. There are always things we haven’t heard about before.
One of the funniest things is that — and I can say this with great confidence today — health is not made in the doctor’s office; it’s made in the kitchen. When people see me today, I say if you’re not willing to change what you’re eating, forget about it, I’m not going to be of any help to you. And if I’m working harder than you, then you’re not going to get better. The primary focus for me is what people are putting into their mouths.”
Diet and Sanitation Are Key Disease-Prevention Strategies
Indeed, diets have always played a key role in disease. Part of the additions made to the 10th anniversary edition of “Dissolving Illusions” is historical dietary and sanitary information.
“It’s always been a huge part of what changed so that human beings weren’t dying of diseases that were circulating,” she says. “Sewage [exposure] was a big part of it. In the mid-1800s, there was so much horse manure and horse urine in the streets in London and New York City. They had literally tons of this stuff sitting in the street, and where people were living.
People were living in apartments and dwellings that literally had cesspools underneath of them. It was part of the house, part of the basement. So, you’d be walking through horse manure, horse urine and dead horses. The average lifespan of a horse was three years back then. We now know horses live into their 30s. That’s a normal lifespan, sometimes longer.
Three years was the average lifespan because even the horses were sickened by what was going on around them. So, what’s going to happen to human beings as a result of that? You think there were fresh farmers markets on that street? No, there weren’t. In fact, some of the people were basically eating rotten meat mixed with saw dust as a sausage. I mean, that was the diet of the average people.
The average person was living in squalor on top of each other and the disease and death rates were extremely high as a result.
Henry Ford did a big favor to the world by bringing out motorcars so we could get these horses and horse dung and horse urine out of the street. That was one of the beginnings. Environmental cleanup was a huge deal … We also had a white slavery system in place then.
If you talk to someone like Catherine Austin Fitts, a financial expert who watches societal changes, she says slavery is the most profitable [business] that has ever existed, and that was true in the mid-1800s. Pregnant women and children with measles were working in coal mines and in bottle factories. They didn’t care that the kid had measles. It was about productivity.
That was all that these owners cared about. So, we had that form of white slavery in that sense that even though you got to go home to your own house, you got a pittance of pay and you couldn’t make ends meet, so you were stressed out. You were a slave to the system. We’re still not really 100% free, but we’re so much better off in terms of what our bodies can accomplish than those people back in the 1700s 1800s.”
More Information
To learn more, be sure to pick up the 10th anniversary update of “Dissolving Illusions: Disease, Vaccines and the Forgotten History,” available on dissolvingillusions.com and Amazon. Buying her book is also the best way to support her work, which is so crucial for our future. The world needs to understand the history behind vaccines to really see the big picture.
“When people read it, even if you just use it as a reference book, it gives you some kind of standpoint to start with when you’re talking to other people,” she says.
“In fact, it’s changed a lot of people’s minds who are pretty much dead set against the idea of no vaccines or limited vaccines. It’s like they start to see it in a different way, because the data are the data. It’s the world’s vital statistics.”
Not only are vaccines harming many people, but by focusing public health efforts on vaccination, so many safer and more effective strategies are overlooked as well. We cannot afford to continue the way we have been, and mandatory mass vaccination of our children is one of the failed strategies that needs to be overhauled if we are to turn our disease statistics around.
For your convenience, I’ve also embedded our previous interview above, where we dive further into some of the dishonest tactics used by the vaccine industry, and why the tetanus vaccine is unnecessary.