Virus
now browsing by category
Garlic Cures 100% of Warts In Clinical Study
© GreenMedInfo LLC. This work is reproduced and distributed with the permission of GreenMedInfo LLC.
Want to learn more from GreenMedInfo? Sign up for the newsletter here:
www.greenmedinfo.com/greenmed/newsletter
Reproduced from original article:
https://greenmedinfo.com/blog/garlic-cures-100-warts-clinical-study
Posted on: Wednesday, March 12th 2025 at 1:30 pm
Written By: Sayer Ji, Founder
This article is copyrighted by GreenMedInfo LLC, 2025
.jpg)
In the first study of its kind, this common herb was found to have remarkable healing results for common warts and corns.
A clinical study published in the International Journal of Dermatology, titled “Healing effect of garlic extract on warts and corns,” reveals the amazing healing properties of garlic extract in healing common warts and corns.
Warts are caused by the virus human papilloma virus (HPV), and corns by pressure of friction. They are some of the most common conditions found in dermatological practice today.
In the new study, peeled garlic was processed to produce either a water or fat based extract. A total of twenty-eight patients with 2-96 warts, nine patients with 1-2 corns, and a control group consisting of five patients with 7-35 warts were enrolled in the study. The study design involved the following methodology:
- In the first phase of the trial, a water extract of garlic was applied twice daily on warts in five patients with 3–5 warts.
- In the second phase, 23 patients with 2–96 warts (all on the hands except for two cases who had plantar warts), and nine patients with 1–2 corns on the feet, were treated by applying a fat-soluble extract of garlic twice daily.
- A control group including two patients with warts and two with corns were treated with a 2:1 ratio of chloroform and methanol solution (the lipid solvent) for a period of 20 days to eliminate the possibility that the treatment results were affected by the solvent.
The treatment results were reported as follows:
- Water extract of garlic: “[F]ive cases received the aqueous garlic extract for 30–40 days, which resulted only in the disappearance of small warts and partial improvement of larger warts. Treatment with the aqueous extract of garlic needed a period of more than 2 months to achieve a partial recovery in the patients.”
- Fat-soluble extract of garlic: “Twenty-three patients with 2–96 warts, and nine patients with 1–2 corns were treated by applying the lipid extract. In this group, complete recovery was observed in all cases with warts after 1–2 weeks of treatment (Fig. 1). Seven out of nine patients with corn(s) showed complete recovery (Fig. 2) while two cases showed marked improvement close to full recovery with no further improvement on continuation of treatment. The period for the treatment of corn(s) in this group was between 10 and 20 days.”
- Chloroform: methanol (control group): The control group showed no improvement.
These study results clearly reveal that the fat-soluble extract of garlic has great potential to heal these common dermatological conditions, with 100% recovery in those with warts, and 80% recovery in those with corns.

(a) Wart on finger. (b) The wart has disappeared after treatment with lipid extract of garlic
The researchers expanded on the implications of their findings by pointing out the relatively inferior results offered through conventional treatments:
“Current treatment for warts in our clinics includes: electrocautery, cryotherapy or application of keratolytics. These approaches are not fully successful, and in some cases warts reappear. In our study, treatment with garlic extract resulted in no recurrence of warts during the follow-up observation period (3–4 months)… Removal of corns by surgery, which is practiced in most clinics, can be painful and costly. Treatment with garlic extract appears to be a more convenient modality.”
Finally, the researchers identified the following four possible mechanisms of garlic’s anti-wart and anti-corn properties:
- Anti-viral – HPV virus is the primary cause of the common wart. Garlic’s anti-viral properties are well established.
- Anti-tumor – warts are actually HPV-associated growths, not unlike benign tumors. Garlic has been found to destroy a wide range of cancer cells. You can view a list of over 160 diseases garlic has been studied to have potential therapeutic value in, including over a dozen different forms of cancer.
- Immune modulatory – The researchers noted that while the mechanism of garlic’s anti-wart and anti-corns activity is unknown, “…enhancement of immunological responses elicited by garlic may be responsible.”
- Fibrinolytic activity – The researchers observed: “Application of garlic extract on a corn caused the removal of the corn from its place. It seems that because of the fibrinolytic effect of garlic, the surrounding fibrin tissue of the corn capsule was lyzed and the capsule was separated from the main tissue.”
For additional research on garlic’s remarkable health properties, take a look at the following pieces of content published on Greenmedinfo.com:
- Garlic Beats Drug in Detoxifying Lead Safely From Body
- Garlic Compares Favorably To A Best-Selling Blood
Originally published: 2014-07-02

Natural Molecules With Anti-Cancer Properties Could Help In These Times Of Turbo Cancers
Reproduced from original article:
https://anamihalceamdphd.substack.com/p/natural-molecules-with-anti-cancer
By: Ana Maria Mihalcea, MD, PhD Feb 25, 2025

We live in a time of turbo cancers and a world that is ever increasing its toxicity and danger for human beings. Both prevention and support for cancer patients is important. Many have been discussing the beneficial effects of Ivermectin and Fenbendazole, but there are so many more molecules available that can additionally support cancer patients and all of those who never want to get cancer.
The Magic of Ivermectin in Oncology
A Drug Made for Animals and Taken by Humans to Treat Cancer: Fenbendazole
Mebendazole: A Cancer Fighting Drug We Find at the Supermarket
I wanted to write about some resources that I have been working with for many years. Sometime in 2019, I met Daniel Stanciu, PhD who at that time was writing the internationally known Cancertreatmentsresearch. He was a physicist who’s life changed dramatically when his former wife developed cancer. He researched almost every natural cancer treatment and repurpose drug that was scientifically available in the world. We used to have many conversations as I have been supporting cancer patients in my integrative clinic and we would discuss novel approaches. You can see our interview from 3 years ago here:
Bringing Light To Novel Cancer Treatment Approaches
Here are some of the many possibilities.
Please read here of 10 cases of advanced cancer cases that achieved complete remission:
10 Cases of Complete Remission from Advanced Cancers after using Supplements or Repurposed Drugs
HCA Garcinia Cambodia combined with Alpha Lipoic Acid
The fruit of G. cambogia contains xanthones, which inhibit preneoplastic lesions in Breast and colon cancer, and induced cancer cell death in mouth, leukemia, breast, gastric, and lung cancer cell lines. Garcinol, inhibited cell proliferation and induced cancer cell death in leukemia, breast, colon, prostate, and pancreatic cancer. Combined therapy with Alpha lipoic acid and HCA has been proposed as an antineoplastic regimen that shifts the metabolism of cancer cells from aerobic glycolysis (the Warburg effect) to respiration. Combined lipoic acid and HCA were evaluated in cancer models with lung carcinoma, melanoma, and bladder carcinoma. Several case series and a case report describe the treatment of patients with advanced metastatic cancer with a combination regimen of alpha lipoic acid and oral HCA.
Curcumin
Curcumin (CUR) is a yellow polyphenolic compound derived from the turmeric plant. It is widely used to treat many types of diseases, including cancers such as those of lung, cervices, prostate, breast, bone and liver. High doses of curcumin of 7 grams per day have induced clinical remission in multiple myeloma and reduction of tumor burden in many other cancers.
The Role of Curcumin in Cancer Treatment
Curcumin acts on the regulation of various immune modulators, including cytokines, cyclooxygenase-2 (COX-2), and reactive oxygen species (ROS), which partly explains its anticancer effects. It also takes part in the downregulation of growth factors, protein kinases, oncogenic molecules and various signaling pathways, such as nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), c-Jun N-terminal kinase (JNK) and signal transducer and activator of transcription 3 (STAT3) signaling.
Quercetin: even more anti-cancer potential than Curcumin?
EGCG
Green tea extracts EGCG a direct anti-tumor effect in several tumor types including chronic lymphocytic leukemia (CLL). Case reports indicate complete remission of CLL with high dose EGCG. EGCG has successfully reduced tumor growth in bladder, colon cancer and been shown to have considerable anti-cancer effects in many other cancer types.
EGCG complete remission Chronic lymphocytic leukemia
Thymoquinone
Thymoquinone which is contained in Black Cumin Seed Oil has been shown to modulate nine out of the ten hallmarks of cancer. Many studies have shown the effects of Nigella sativa on various cancer cells, and the list is long offering up over 57 reviewed papers on the subject finding black cumin to be effective against cancers such as blood, breast, colon, pancreatic, lung, leukemia, skin, fibrosarcoma, renal, prostate, and cervical cancer. It has profound anti-inflammatory effects.
Thymoquinone in the clinical treatment of cancer: Fact or fiction?
Thymoquinone: A Promising Therapeutic Agent for the Treatment of Colorectal Cancer
Citrus Bergamont
Citrus Bergamont (CR) inhibits via the malevolate pathway of cholesterol and fatty acid synthesis that cancers use to grow. The uptake of fatty acids not only by the tumor cells but also the connective tissue cells necessary for building new cancer cells can affect continued tumor progression. CR inhibits this uptake and has been shown to inhibit tumor cell growth in colon cancer. It also inhibits cancer stem cells, and important mechanism that prevents metastatic disease. Statin drugs have been able to inhibit cancer cell growth but have significant side effects. CR exhibits similar benefits of statin drugs without side effects.
Anti Cholesterol Strategy to Fight Cancer
Grape Seed Extract
The key reason Grape Seed Extract is used as a food supplement is its high content of Oligomeric Proanthocyanidins (OPC), powerful substances found in the bark of trees, fruit skins, seeds, and leaves. Natural sources of OPCs include grape seeds and skins, blueberries, cranberries, and coffee. Proanthocyanidins are developed by plants as a defense against biotic and abiotic stressors, protecting them from pathogens and predators. The potential benefits of Proanthocyanidins are extensively studied, covering cardiovascular health, inflammation, skin health, immunity, brain health, gastrointestinal health, metabolic syndrome, microbial infections, and oncology.
These benefits are likely related to their impact on the microbiome, increasing diversity and improving the balance of gut microbes (2).
While there are various areas where OPCs can help, those that stand out the most are:
1. Microbial infections
Pathogen Adhesion: Proanthocyanidins may represent a good support to help the body maintain a healthy response to the adhesion of pathogens to the mucosal surfaces, such as the urinary tract epithelium;
Biofilm Formation: microbes regulate through biofilm formation for survival from host defense, which is often found difficult in its eradication with simple anti-microbial agents. Research indicates Proanthocyanidins may represent a good support for the human body when it comes to adherence, motility and biofilm formation of major microbial infections including Candida albicans
Viruses: Proanthocyanidins maintain a healthy response to external agents (7).
2. Oncology support
Unhealthy Stem Cells: Proanthocyanidins may help reverse EMT through Suppression of TGF- β Signaling Pathway
Angiogenesis: Grape seed proanthocyanidins inhibit MMP-2 and MMP-9 secretion, VEGF and angiopoietin 1 signaling, to inhibit angiogenesis
Hypoxia-Inducible Factors: Proanthocyanidins suppress HIF-1α-dependent pathway
3. Inflammation and pain
Gut Microbiota: Proanthocyanidins may contribute to maintaining healthy gut microbiota, which is essential for a well-functioning immune system.
Neuropathic Pain: Proanthocyanidins have been shown to help suppress matrix metalloproteinase-9/2 (11), inflammasomes in macrophages (12), and inhibiting the activity of pyramidal cells in the insular cortex
C-Reactive Protein (CRP) – marker of inflammation was lowered.
NF-κB Signaling Pathway: Inactivating the NF-κB signaling, and downregulating pro-inflammatory cytokines and mediators such as TNF-α, IL-6, and COX-2
Chrysin
Chrysin is a flavonoid present in various natural sources such as honey, propolis, and certain plant species, exhibiting varying concentrations across different sources. For example, honeydew honey contains approximately 0.10mg/kg of Chrysin, while forest honeys boast a higher concentration of around. Chrysin has gained considerable attention during the recent years due to its outstanding potential to add value to life in multiple key areas of health, including
1. Brain health
Chrysin has been identified as a potential MAO (Monoamine Oxidase) inhibitor and GABA mimetic. MAO is one of the few enzymes involved in the process of dopamine metabolization. As such, Chrysin may offer significant support in a variety of brain related health challenges, such as Alzheimer’s disease, Parkinson’s disease, depression, anxiety, brain tumors, epilepsy, multiple sclerosis, traumatic brain injury, spinal cord injury, and ischemic stroke.
2. Oncology support
Chrysin demonstrates not only modulation of MAO-B but also stronger inhibition of MAO-A, which has implications in oncology (4). Recent research from UCLA suggests that substances blocking MAO-A can enhance the activity of T-cells in the immune system and inhibit tumor-associated macrophages, potentially aiding in immune response against tumors. Multiple scientific studies have suggested that Chrysin has an important potential to suppress the enzyme aromatase (CYP19) relevant when it comes to unhealthy breast cells, since aromatase is the enzyme responsible for the conversion of testosterone into estrogen.
3. Other benefits
Testosterone support: Due to its aromatase inhibition potential, Chrysin is also expected to represent good support for a healthy testosterone level.
Liver and Kidney support: Chrysin, has been also suggested to represent a relevant liver and kidney support in the presence of natural or chemical toxins
Chrysin a promising anticancer agent: recent perspectives
Modified Citrus Pectin
Modified Citrus Pectin is a soluble fiber derived from citrus peels, processed to enhance its absorption and availability to the body’s cells. In its natural form, pectin is a large molecule that is not absorbed by the human digestive tract. Modified citrus pectin is a pectin form that undergoes enzymatic processing to reduce its molecular weight and size. These are smaller particles, called modified citrus pectin, are more easily absorbed through the intestinal lining into the bloodstream. Once it has entered the circulation, Modified Citrus Pectin binds to and blocks galectin-3, a protein that fuels inflammation, hardens tissues and organs—including the arteries—and can give rise to a number of serious health impacts throughout the body.Galectin-3 is also involved with several cellular activities, which include apoptosis, cell migration, proliferation, angiogenesis and epithelial–mesenchymal transition (EMT) and it is therefore known to play a key role in the spread and metastasis process. In unhealthy cells, Galectin-3 over-expressing cells show an increased migration, whereas down-regulation ofgalectin-3 expression results in decreased migratory and invasive characteristics of unhealthy cells. Therefore, Modified Citrus Pectin, as a galectin-3 inhibitor, is expected to support the body in the fight against the spread of unhealthy cells.
Modified Citrus Pectin also possesses chelating properties, enabling it to bind with heavy metals and toxins in the body and facilitate their excretion. This enhances the body’s detoxification abilities.
I have written about the properties of Galectin induced turbo cancers from Lipid nanoparticles and their inhibition by Curcumen, Berberine and Citrus Pectin here:
Glycolysis Inhibitors
Drugs and Supplements that Block Fermentation and Help Fight Cancer
Glucose Absorption Inhibitors to Inhibit Tumor Growth
Glycolysis, the process of breaking down glucose for energy, is essential for cellular function. It is a fundamental metabolic pathway that occurs in the cytoplasm of cells, where glucose (a six-carbon sugar) is broken down into two molecules of pyruvate. This process generates energy in the form of ATP (adenosine triphosphate) and NADH. Glycolysis consists of ten enzymatic steps and is the first stage of both aerobic and anaerobic respiration. Unhealthy cells, have Glycolysis upregulated
(“Warburg effect”) insuring energy production as part of the Fermentation process, in the absence of oxygen (anaerobic process).
Downregulating glycolysis can:
Promote metabolic flexibility, encouraging the body to use other energy pathways, such as fat oxidation. Indeed, it has been suggested that Glycolysis inhibitors can support Ketogenic Diet. Reduce lactate buildup, helping to maintain better cellular function and reduce fatigue as well as supporting the normal function of the immune system. Support overall cellular health, especially in cases of metabolic stress.
Glycolysis Inhibithree
Targeting 3 Key Steps in Glycolysis
PHLORIZIN – derived from the bark of apple trees, natural compound studied for its role in glucose transport.
TANSHINONE IIA – found in the Chinese traditional herb Danshen (Salvia miltiorrhiza), a natural compound studied in relation to HK2 (Hexokinase II).
Shikonin – a natural naphthoquinone compound from the root of Zi Cao (Lithospermum erythrorhizon), a traditional Chinese herb, studied for its role in cellular processes like Pyruvate Kinase M2(PKM2) activity.
AHCC®
Is one of World’s leading immune health supplements.
AHCC® contains an unique Shiitake-Mycelia extract discovered by Japanese scientists in 1989. Today, its potential is supported by over 30 scientific studies, including clinical studies in humans. AHCC® is extracted from Shiitake mushrooms. However, what makes AHCC® different compared to other Shiitake extracts is that it is grown in fermenters. During this process, mushroom enzymes modify the natural polysaccharides to generate active compounds called partially acetylated alpha-glucans. These partially acetylated alpha-glucans are responsible for and contribute to the superior absorption and strong clinical efficacy of AHCC®. Indeed, AHCC® outstanding results have been observed in relation to mechanisms & health challenges such as: Natural Killer and T- cell number and activity, Human Papillomavirus infections. Various Bacterial, Fungal and Viral infections
Genistein
Genistein is a naturally occurring isoflavone found in plants like soy and Sophora japonica, known for its antioxidant and anti-inflammatory properties. It plays a significant role in supporting women’s health, particularly in hormonal balance and bone strength, helping to reduce post menopausal side effects. Additionally, Genistein is being studied for its potential role in oncology, where its influence on cellular pathways and estrogen receptors may offer protective benefits in cancer management. Its dual action makes it valuable for both general well-being and specific therapeutic areas.
Genistein is a potent isoflavone that exerts significant effects on various intracellular mechanisms. It is known to modulate cell signaling pathways, such as the PI3K/Akt and MAPK pathways, which are crucial for cell survival, growth, and differentiation. Genistein also influences apoptosis (programmed cell death) by regulating Bcl-2 proteins and promoting the activation of caspases. Additionally, it affects estrogen receptors and can inhibit the activity of enzymes like tyrosine kinases, as well as topoisomerase II reducing excessive cell proliferation. These mechanisms make Genistein of interest for both hormonal balance and potential anticancer therapies.
Genistein as a Potential Tool to Fight Metastasis & More
Boswellia AKBA
Historically, Boswellia has been valued not only in the context of cultural rituals for its soothing properties and fragrant aroma , but also for its medicinal properties, traditionally used in Ayurvedic medicine for its anti-inflammatory properties. The active compounds, Boswellic acids, are known to help support joint health, reduce inflammation, and have been studied for their potential benefits related to health conditions like arthritis and inflammatory bowel disease. Scientific studies have identified Boswellic Acids, particularly AKBA (Acetyl-11-keto-beta-boswellic acid), as key compounds responsible for its health benefits.
Anti-cancer properties of boswellic acids: mechanism of action as anti-cancerous agent
The mechanisms of activity of BAs comprise a variety of targets, including the enzymes of angiogenesis and others such as topoisomerases, 5-lipoxygenase (5-LO), cytochrome P450, and mitogen-activated protein kinase (MAPK, especially p38) which are either promoted or inhibited by BAs
Apigenin
Apigenin can induce apoptotic cancer cell death via increasing ROS generation in cancer cells, the downregulation of anti-apoptotic factors Bcl-2 and Bcl-xl as well as the up-regulation of apoptotic factors Bax and Bim.
Apigenin can induce cell cycle arrest at the G2/M and S phases.
In suppressing metastasis of cancer cells, apigenin administration interferes with the PI3K/Akt/mTOR signaling pathway as well as suppresses the expression of MMP-9, a factor involved in the progression and invasion of cancer cells.
Most studies indicate activity in Breast Cancer, Lung Cancer, Colon Cancer, Skin Cancer, Pancreatic Cancer, Cervical Cancer, Prostate Cancer. Diminished the incidence of UV light-induced cancers.
Apiginin is a great Nootropic which improves cognitive function and is neuroprotective. It also promotes relaxation with slight sedative effect, supports sleep and ameliorates Post-Stroke Cognitive Deficits.
Glutamine Inhibition
Most Cancer Types are dependent on Glutamine. Glutamine metabolism is upregulated in many forms of cancer as it is required for Nucleotides, Glutathione, ATP and Lipid production. Prostate tumors, Brain tumors, Triple Negative Breast tumors, Leukemia are known to be most dependent on Glutamine Mutations in the genes IDH1 and IDH2, which also change how glutamine products are used in a cell, are common in certain types of brain cancer and leukemia.
Glutamine Inhibition increases the effectiveness of Metformin and 2DG against tumors cells. BRAF inhibition causes a shift of cancer cells to glutamine for resistance & survival. GLS inhibition restores sensitivity to the EGFR inhibitor erlotinib in cells that have developed resistance.
Glutamine Inhibifour
Glutamine Inhibifour is the first food supplement designed with the GLUTAMINOLYISIS pathway in mind.
Targeting glutamine metabolism as a therapeutic strategy for cancer
Omega-3 Fatty Acids, Budwig Diet & their Antitumor Activity
Baicalein
Potential to modulate PI3K/AKT/mTOR, Wnt/β-catenin, MAPK, NF-κB, Notch, ROS, and Shh signaling. Anti-migration and anti-invasion potential. Anti-angiogenesis potential due to inhibition of 12-Lipoxygenase. Outstanding Iron chelator and anti-Fenton property. Inhibits TLR4 and the downstream HIF‐1α and VEGF expressions
Breast Cancer, Lung Cancer, Ovarian Cancer, Colo Rectal Cancer
There are many more possibilities, and you can find out more on the cancertreatmentsresearch.com site.
___________________________________________________________________________
Daniel proceeded to create MCS formulas and design supplements that help cancer patients, while omitting any fillers, toxic nanoparticles. 50% of the proceeds continue to go to research natural cancer solutions. His supplements have been of such tremendous quality that they are used in clinical trials by very esteemed cancer institutions around the world. I have been listed on his site as an integrative Oncology consultant for many years and my book Light Medicine – A New Paradigm – The Science of Light, Spirit and Longevity due to its case reports of using integrative approaches to support cancer patients effectively. I use the MCS formula supplements in my clinic while treating patients with many different natural intravenous molecules in collaboration with their Oncologist. He has branched into antiaging and longevity which is my specialty. Now that we have the good news that Robert F Kennedy Jr has been confirmed, and we have so much needed shake up with our current administration, we are looking into a much more hopeful future in which doctors who use natural cancer treatments supportively may not be hunted by the governmental agencies and specialty boards. There are a lot of possibilities for help. Many pharmaceutical repurpose drugs can be replaced with natural supplements that have equivalent effect. For example instead of Metformin use Berberine, instead of a Statin, which is a mitochondrial toxin, use Citrus Bergamot. In my clinic I use many of these molecules intravenously as well for shedding related chronic illness with remarkable results, like Resveratrol, Quercetin, Curcumin, Artemesinin, EGCG etc. Any cancer patient can use Glycolysis and Glutamate inhibition.

Vitamin C does work for colds – but UK authorities didn’t report it
Orthomolecular Medicine News Service, February 18, 2025
Reproduced from original OMNS article (OrthoMolecular News Service):
http://orthomolecular.org/
Subscribe to the free Orthomolecular Newsletter: http://orthomolecular.org/subscribe.html
Go to the OMNS Archive: http://orthomolecular.org/resources/omns/index.shtml
by Patrick Holford
A new review of vitamin C evidence concludes that doses of vitamin C above 1 gram decreases cold severity and doses of at least 6 grams, ideally 8 grams, during a cold reduced duration considerably, halving recovery time if you take 8 grams. [1]
A previous UK placebo-controlled trial illustrates the meaningful clinical difference between the number of colds, cold duration and severity. [2] This trial comprised 168 volunteers who were randomized to receive a placebo or vitamin C (2 x 500 mg daily) over a 60-day winter period. The vitamin C group had fewer colds (37 vs 50, P = 0.05), and even fewer virally challenged ‘cold’ days (85 vs 178, P=0.03) and a shorter duration of severe symptom days (1.8 vs 3.1 days, P = 0.03). The number of participants who had two colds during the trial was significantly reduced (2/84 on vitamin C vs 16/84 in the placebo group; P = 0.04). In summary, cold symptoms have been shown to be less severe and resolve more quickly with oral vitamin C with a dose-dependent effect.
Higher doses, such as 1 gram per hour, which Dr Linus Pauling first recommended to achieve the same blood level of vitamin C of animals who make during the viral infection, may be more effective but no trials have been done at that level. Pharmacokinetic studies in healthy volunteers support a 200 mg daily dose to produce a plasma level of circa 70 to 90 µmol/l. [3] Higher intakes of vitamin C are, however, likely to be needed during viral infections with 2-3 g maintaining normal plasma levels between 60 and 80 µmol/l, [4] taken every 2 to 4 hours, as viral infection depletes vitamin C. A similar finding occurred in covid-19 patients for whom plasma concentrations of vitamin C in most of these patients were reported to be very low with 70-80% of the patients having hypovitaminosis C (plasma concentration <23 µmol/L). [5,6] Whether higher plasma levels higher than 60 to 80µmol/L have additional benefit is yet to be determined but would be consistent with the results of clinical trials.
Professor of Public Health, Dr. Harri Hemila from the University if Helsinki, who authored this review has also reanalyzed the seminal Sheffield Study in the UK, back in the 1940’s. [7]
In the study 10 participants were “deprived” and not given vitamin C supplements, 7 participants were administered 10 mg/day vitamin C as a supplement, and 3 participants were administered 70 mg/day.
Colds lasted on average 6 days during vitamin C deprivation, compared with 3 days on the 10-70 mg/day dosage. Thus, deprivation nearly doubled the duration of colds. Jowett concluded that “such evidence as there is, however, definitely confirms the hypothesis that the absence of vitamin C tended to cause colds to last longer”.
The reanalysed results show that vitamin C deprivation increased the duration of colds on average by 77% (P = 0.014). Vitamin C deprivation decreased the recovery rate from colds by 60% (P = 0.008) and extended the duration of 1 day colds by 2.2 days. (95% CI 1.0 to 5.4 days).
“The finding that vitamin C deprivation extended the duration of colds was not reported in the summaries of the trial published in the Lancet (1948) and in the Proceedings of the Nutrition Society (1953). In addition, this finding is also not mentioned in the current UK recommendations for vitamin C. As a consequence, readers have not been fully informed about the common cold results of the Sheffield trial for several decades.” Says Professor Hemila. The Lancet was the UK’s leading medical journal at that time.
References
1. Hemilä H, Chalker E (2025) Vitamin C for the common cold and pneumonia. Pol Arch Intern Med. 2025:Jan 13:16926. https://doi.org/10.20452/pamw.16926
2. Van Straten M, Josling P (2002) Preventing the common cold with a vitamin C supplement: a double-blind, placebo-controlled survey. Adv Ther. 19:151-159. https://pubmed.ncbi.nlm.nih.gov/12201356 https://www.researchgate.net/profile/Peter-Josling/publication/11187865
3. Levine M, Conry-Cantilena C, Wang Y, et al. (1996) Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance. PNAS USA, 93:3704-3709. https://pubmed.ncbi.nlm.nih.gov/8623000; see also Levine M, Wang Y, Padayatty SJ, Morrow J (2001) A new recommended dietary allowance of vitamin C for healthy young women. PNAS USA, 98:9842-9846. https://pubmed.ncbi.nlm.nih.gov/11504949
4. de Grooth HJ, Manubulu-Choo WP, Zandvliet AS, et al. (2018) Vitamin-C pharmacokinetics in critically ill patients: a randomized trial of four intravenous regimens. Chest, 153:1368-1377. https://pubmed.ncbi.nlm.nih.gov/29522710; see also Hume R, Weyers E (1973) Changes in leucocyte ascorbic acid during the common cold. Scott Med J. 18:3-7. https://journals.sagepub.com/doi/abs/10.1177/003693307301800102
5. Arvinte C, Singh M, Marik PE (2020) Serum Levels of Vitamin C and Vitamin D in a Cohort of Critically Ill COVID-19 Patients of a North American Community Hospital Intensive Care Unit in May 2020: A Pilot Study. Med Drug Discov.8:100064. https://doi.org/10.1016/j.medidd.2020.100064
6. Tomasa-Irriguible TM, Bielsa-Berrocal L (2021) COVID-19: Up to 82% critically ill patients had low Vitamin C values. Nutr J. 20:66. https://doi.org/10.1186/s12937-021-00727-z.
7. Hemilä H (2025) Effect of vitamin C deprivation on the duration of colds in the Sheffield study (1953): a statistical analysis. Zenodo. Jan 22, 2025 online. https://doi.org/10.5281/zenodo.14717361
Orthomolecular Medicine
Orthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org
Find a Doctor
To locate an orthomolecular physician near you: http://orthomolecular.org/resources/omns/v06n09.shtml
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Jennifer L. Aliano, M.S., L.Ac., C.C.N. (USA)
Albert G. B. Amoa, MB.Ch.B, Ph.D. (Ghana)
Seth Ayettey, M.B., Ch.B., Ph.D. (Ghana)
Ilyès Baghli, M.D. (Algeria)
Greg Beattie, Author (Australia)
Barry Breger, M.D. (Canada)
Ian Brighthope, MBBS, FACNEM (Australia)
Gilbert Henri Crussol, D.M.D. (Spain)
Carolyn Dean, M.D., N.D. (USA)
Ian Dettman, Ph.D. (Australia)
Susan R. Downs, M.D., M.P.H. (USA)
Ron Ehrlich, B.D.S. (Australia)
Hugo Galindo, M.D. (Colombia)
Gary S. Goldman, Ph.D. (USA)
William B. Grant, Ph.D. (USA)
Claus Hancke, MD, FACAM (Denmark)
Patrick Holford, BSc (United Kingdom)
Ron Hunninghake, M.D. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Dwight Kalita, Ph.D. (USA)
Felix I. D. Konotey-Ahulu, M.D., FRCP (Ghana)
Peter H. Lauda, M.D. (Austria)
Fabrice Leu, N.D., (Switzerland)
Alan Lien, Ph.D. (Taiwan)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Pedro Gonzalez Lombana, M.D., Ph.D. (Colombia)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Juan Manuel Martinez, M.D. (Colombia)
Mignonne Mary, M.D. (USA)
Dr.Aarti Midha M.D., ABAARM (India)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Sarah Myhill, MB, BS (United Kingdom)
Tahar Naili, M.D. (Algeria)
Zhiyong Peng, M.D. (China)
Pawel Pludowski, M.D. (Poland)
Isabella Akyinbah Quakyi, Ph.D. (Ghana)
Selvam Rengasamy, MBBS, FRCOG (Malaysia)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
Thomas N. Seyfried, Ph.D. (USA)
Han Ping Shi, M.D., Ph.D. (China)
T.E. Gabriel Stewart, M.B.B.CH. (Ireland)
Jagan Nathan Vamanan, M.D. (India)
Dr. Sunil Wimalawansa, M.D., Ph.D. (Sri Lanka)
Andrew W. Saul, Ph.D. (USA), Founding Editor
Richard Cheng, M.D., Ph.D. (USA), Editor-In-Chief
Associate Editor: Robert G. Smith, Ph.D. (USA)
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Editor, Chinese Edition: Richard Cheng, M.D., Ph.D. (USA)
Editor, Norwegian Edition: Dag Viljen Poleszynski, Ph.D. (Norway)
Editor, Arabic Edition: Moustafa Kamel, R.Ph, P.G.C.M (Egypt)
Editor, Korean Edition: Hyoungjoo Shin, M.D. (South Korea)
Editor, Spanish Edition: Sonia Rita Rial, PhD (Argentina)
Editor, German Edition: Bernhard Welker, M.D. (Germany)
Associate Editor, German Edition: Gerhard Dachtler, M.Eng. (Germany)
Assistant Editor: Michael Passwater (USA)
Contributing Editor: Thomas E. Levy, M.D., J.D. (USA)
Contributing Editor: Damien Downing, M.B.B.S., M.R.S.B. (United Kingdom)
Contributing Editor: W. Todd Penberthy, Ph.D. (USA)
Contributing Editor: Ken Walker, M.D. (Canada)
Contributing Editor: Michael J. Gonzalez, N.M.D., Ph.D. (Puerto Rico)
Technology Editor: Michael S. Stewart, B.Sc.C.S. (USA)
Associate Technology Editor: Robert C. Kennedy, M.S. (USA)
Legal Consultant: Jason M. Saul, JD (USA)
Comments and media contact: editor@orthomolecular.org OMNS welcomes but is unable to respond to individual reader emails. Reader comments become the property of OMNS and may or may not be used for publication.
Riordan Clinic | Orthomolecular.org
3100 N Hillside Ave
Wichita, Kansas 67219
United States
The History and Therapeutic Mechanisms Of Chlorine Dioxide
Reproduced from original article:
https://pierrekorymedicalmusings.com/p/the-history-and-therapeutic-mechanisms
Pierre Kory’s Medical Musings
Chlorine dioxide was discovered over 200 years ago. It’s use has steadily expanded into many industries and therapeutic applications despite a near global regulatory blockade on clinical research.
Jan 27, 2025
I believe that my writings on chlorine dioxide are the most important (and the most dangerous) work I have yet done on Substack. Although several experts have written extensively on this topic previously (here, here, and here), this similar effort of mine simply results from my wish to become as knowledgeable as possible about this critically important therapeutic (there is no better way to do so than personally researching and writing about a topic).
This is the 3rd in my ongoing series of posts. In the first two I presented the political context in which chlorine dioxide has been attacked during Covid (“Trump’s Bleach Conference”) and in the 2nd post I detailed the success achieved by Bolivia’s national chlorine dioxide program against Covid.
In this post I will review its discovery, chemical properties, industrial applications, and therapeutic mechanisms. Upcoming posts will cover the history of the attacks faced by the pioneering researchers and practitioners, followed by a review of the safety studies of oral ingestion and a compilation of studies showing efficacy in a number of diseases. Be sure to subscribe so as not to miss out on these critical upcoming posts.
Ultimately, what me and my growing network of clinical and scientific experts of this therapeutic compound want to achieve, is for the FDA (and the copycat regulatory agencies worldwide) to lift its restrictions on performing clinical research trials of chlorine dioxide in human diseases. If anyone from MAHA is reading this right now (and I know some are), please add chlorine dioxide (and DMSO) to the list of therapies currently being suppressed by the FDA that need to be reversed (RFK Jr listed more than a dozen other such therapies in the below recent tweet):

Note that, in the below, many (but not all) references were found from the superlative theuniversalantidote.com’s website, from their “interactive reference guidebook” document.
Chlorine Dioxide – What It is, What It Isn’t
Chlorine Dioxide is a small, volatile and strong molecule consisting of 1 chlorine atom and 2 oxygen atoms.
- It is a gas at normal temperatures and pressures.
- Yellowish/green color and has an odor similar to that of chlorine.
- Denser than air and is water soluble at standard temperatures and pressures up to 2500ppm.
- Explosive in air at concentrations >10%. It is therefore normally generated in-situ (on-site) within an aqueous solution at <0.3%
- Chlorine dioxide is a biocide. This means it kills all bacteria, viruses, and fungus on contact through a process of oxidization.
Chlorine dioxide was initially discovered in 1814 by Sir Humphrey Davy and was commercially produced in 1940 as a bleaching agent. It is labeled as a strong oxidizing agent, microbicide, and antiseptic. Based on these references here and here, chlorine dioxide is also known to have the ability to “neutralize various toxins, pesticides, herbicides, and pharmaceuticals contaminating drinking water.”
As an added bonus, it can do all of that without producing any harmful organic compounds as occurs with nearly all other disinfectants (like bleach – which contrary to FDA “warnings,” chlorine dioxide certainly is not).
Chlorine dioxide is more effective as a disinfectant than chlorine in most circumstances against waterborne pathogenic agents such as viruses, bacteria, and protozoa – including the cysts of Giardia and the oocysts of Cryptosporidium.
Chlorine dioxide has been extensively studied within multiple fields (commercial, industrial, healthcare) and by multiple entities including: EPA, HHS, USDA, CDC, NIH, NASA, DOD, independent laboratories, and universities worldwide.
Chlorine dioxide is registered as a sterilizer and biocide and is used to sterilize medical facilities and laboratories including BSL-3 and BSL-4 labs which handle the world’s most deadly pathogens. It was used to decontaminate the Senate offices in 2001 after the anthrax attack, and was also used in Ebola hot spots.
From this systematic review paper on chlorine dioxide as a disinfectant:
Different chemical structures with properties of disinfectants have been identified. These chemical structures include alcohol, aldehydes, anilides, biguanides, bisphenols, diamidines, halogen-releasing agents, halophenols, heavy metal derivatives, peroxygens, quaternary ammonium compounds, phenols, and cresols. However, each disinfectant attacks different target areas of the micro-organisms. Disinfectants can be divided into two broad groups: oxidizing and non-oxidizing disinfectants. Disinfectants containing halogens such as chlorine, iodine, and oxygen releasing materials are called oxidizing disinfectants, while disinfectants that bond to structures such as quaternary ammonium compounds and amphoterics are known as non-oxidizing disinfectants.
Oxidizing agents like chlorine dioxide are chemical compounds that accept electrons from “electron donors.” This is important because relative to chlorine dioxide, all pathogens (disease causing organisms or substances) are electron donors.
So what happens to chlorine dioxide after it reacts and oxidizes the pathogens? In aqueous systems, chlorine dioxide eventually decomposes into generally safe byproducts that naturally occur in our environment, i.e. chloride ions (like in table salt), oxygen (O₂), and other non-toxic residues.
From Chat GPT when asked to contrast chlorine dioxide with bleach:
Chlorine dioxide and bleach (sodium hypochlorite) are both powerful oxidizing agents commonly used as disinfectants, but they differ significantly in their chemical structure, mechanism of action, and applications. Here’s how they compare:
1. Chemical Composition
- Chlorine Dioxide (ClO₂): A gas at room temperature, typically dissolved in water for use. It is a single molecule composed of one chlorine atom and two oxygen atoms.
- Bleach (Sodium Hypochlorite, NaOCl): A liquid solution containing sodium hypochlorite as the active ingredient, along with water and small amounts of other chemicals.
2. Mechanism of Action
- Chlorine Dioxide: Kills microorganisms by disrupting their metabolic processes and breaking down cell membranes and proteins. It primarily reacts with organic matter through oxidation.
- Bleach: Also acts as an oxidizer, generating hypochlorous acid (HOCl) in water, which destroys bacteria and viruses by disrupting their enzymes and proteins.
3. By-products
- Chlorine Dioxide: Produces fewer harmful by-products, primarily chlorite and chlorate ions (initially), which are less persistent in water systems compared to bleach by-products.
- Bleach: Can produce potentially harmful chlorinated organic compounds (e.g., trihalomethanes and chloramines), especially when reacting with organic matter in water. (Editorial note: this is extremely important, trihalomethanes are suspected carcinogenic disinfection by-products[ associated with chlorination of naturally occurring organics in raw water.
4. Effectiveness
- Chlorine Dioxide: Remains effective over a wide pH range (4–10) and is less affected by the presence of organic matter, making it suitable for challenging disinfection tasks.
- Bleach: Its efficacy decreases significantly outside a pH range of 6–8 and in the presence of organic matter.
5. Applications
- Chlorine Dioxide:
- Water treatment (municipal, industrial, and potable water systems).
- Food and beverage sanitation.
- Medical disinfection and biofilm removal.
- Bleach:
- Household cleaning and laundry.
- Pool and spa disinfection.
- Surface disinfection in healthcare and other settings.
6. Safety and Stability
- Chlorine Dioxide: Typically generated on-site because it is unstable as a concentrated gas and can decompose explosively. However, it is considered safer for certain applications due to fewer toxic by-products.
- Bleach: Stable in liquid form but degrades over time, particularly when exposed to light and heat. It has a strong, recognizable smell and can be irritating to skin and respiratory systems.
7. Odor and Residue
- Chlorine Dioxide: Has a less pronounced odor and does not leave a strong chemical residue or taste in treated water.
- Bleach: Has a strong chlorine smell and can leave noticeable chemical residues.
Summary:
While both are effective disinfectants, chlorine dioxide is often preferred for applications requiring minimal by-products and effectiveness in diverse conditions, whereas bleach is more common for general-purpose household and industrial disinfection.
TIMELINE OF ITS ADOPTION ACROSS INDUSTRIES
Taken from pioneer Jim Humble’s website, here I provide a short paraphrased history of its use in industry where I also dug up the references:
1811: Chlorine dioxide is discovered by Sir Humphrey Davy, when he adds sulfuric acid (H2SO4) to potassium chlorate (KClO3). In the early 1900’s it was recognized as an antimicrobial biocide and became known for its disinfectant properties.
1930’s: Due to concerns about the logistics of safely transporting the gas, sodium chlorite began to be manufactured as a relatively safe precursor chemical, and the industries using chlorine dioxide would then generate the gas onsite as needed. Because of chlorine dioxide’s solubility in water, it starts being used as a water treatment.
1944: First commercial application. Used as a biocide/taste and odor control agent in domestic water at Niagara Falls in the USA.
1950’s: Increasing use of chlorine dioxide in water treatment plants and swimming pools in the U.S.A. Likewise it is discovered that chlorine dioxide destroys biofilm, the algal slime that collects in cooling towers, among other places and harbors harmful bacteria. Chlorine bleach by contrast cannot kill biofilm.
1956: Brussels, Belgium, switches to chlorine dioxide from chlorine for its drinking water disinfection operations. This marks the first large scale use of chlorine dioxide for potable water treatment.
1967: The Environmental Protection Agency (EPA) of the United States first registers chlorine dioxide as a disinfectant and sanitizer. The registration is for chlorine dioxide in the liquid form. Indicated uses include food processing (!), handling and storage plants, bottling plants, washing fruit and vegetables (!), sanitizing water, controlling odors, and treating medical wastes.
1970’s: The EPA begins recommending using chlorine dioxide instead of chlorine bleach to treat water. Hundreds of municipal water systems successfully convert to chlorine dioxide. This happens across the United States and Europe; more so for the latter. The conversion is catalyzed by a safer environmental profile of chlorine dioxide over chlorine, because chlorine dioxide does not produce any harmful byproducts, as does chlorine bleach.
1977: Three thousand municipal water systems achieve biological control using chlorine dioxide (EPA document here)
1980’s: Chlorine dioxide gradually replaces chlorine in many industries – in the pulp and paper industry as a bleaching agent, in industrial water treatment as a biocide and as an odor control agent, in food processing as a sanitizer.
1983: The EPA recommends chlorine dioxide as a solution for the problem of trihalomethanes (THMs). When chlorine is used to disinfect water and make it potable (chlorination), THMs are produced as a by-product. THMs have been linked to cancer (i.e., they are carcinogenic). Chlorine dioxide does not produce THMs.
1988: The EPA registers chlorine dioxide as a sterilizer. This means chlorine dioxide is both safe and effective to use in hospitals, healthcare facilities, and laboratories.
1990: Use of chlorine dioxide as a disinfectant, sanitizer and sterilizer grows across many industries and countries. Some of the industries are the beverage industry, fruit and vegetable processing plants, pulp and paper industries, and industrial waste treatment sites. These industries are spread across the United States, the United Kingdom and Europe.
2001: The Federal Emergency Management Agency (FEMA) and other government agencies use chlorine dioxide to decontaminate buildings contaminated with Anthrax. The chlorine dioxide was completely effective against the tiny Anthrax spores. The buildings, walls and furnishings suffered no damage from the treatment.
2005: FEMA again uses chlorine dioxide. It is used to eradicate mold infestations in homes damaged by the flood waters from Hurricane Katrina. After a 12-hour treatment, a New Orleans restaurant is able to banish all mold inside without rebuilding.
2010: The United States Food and Drug Administration issue a warning on using the chlorine dioxide formulation called Miracle Mineral Solution (MMS – made by combining sodium chlorite with hydrochloric acid) and pioneered by Jim Humble in his numerous treatment protocols. The FDA repeatedly describes it as industrial bleach while at the same time approving chlorine dioxide for use in mouthwashes, toothpastes, and as a food service disinfectant, citing it as being a better alternative than chlorine.
2014: The Centers for Disease Control (CDC) registers ProKure V and PERFORMACIDE® as disinfectants against the Ebola virus. Both contain chlorine dioxide. ProKure V claims it “begins to kill pathogens in a matter of seconds, whereas other commonly used, more traditional disinfectants take minutes. The rapid speed in which ProKure V kills pathogens makes it a product of choice for helping contain infectious-disease outbreaks and keeping public facilities cleaner and safer for everyone.” Chlorine dioxide is a potent virucide.”
EFFICACY AND SAFETY AS A BIOCIDE
Chlorine dioxide is one of, if not the fastest known and “complete spectrum” disinfectants, killing all forms of bacteria (aerobic, anaerobic, gram positive and negative), viruses, fungi and yeast, typically within a minute of contact, (spores a little longer), and notably without damage to animal cells, or even tissue culture cells.
In this mouse study (know that mice are more sensitive than humans to toxicities for many but not all compounds), they found that at concentrations between 5 and 20 ppm (this concentration becomes highly relevant in a later post when I discuss safety of oral treatment dose concentrations), chlorine dioxide killed almost all of the bacteria and fungi present while no damage to lung cells, eyes, or other organs was observed, even when 40ppm was added to their drinking water sub-chronically. The study concluded “chlorine dioxide showed favorable disinfection activity and a higher safety profile tendency than in previous reports.”
This is a very short list of papers showing in vitro and/or in vivo (animals) efficacy against a number of viruses and bacteria (more on this in a later post).
Typhoid, Norovirus, Hepatitis C virus, HPV, HIV, Influenza A Virus, E.Coli, Listeria, Rotavirus, Mycobacterium Avium, Hepatitis A Virus, staph aureus, also hospital pathogens like Acinetobacter baumannii, Escherichia coli, Enterococcus faecalis, Mycobacterium smegmatis, and Staphylococcus aureus.
Moving away from in vitro data in order to show that it can cure infectious disease in animals (in vivo study), in a randomized controlled trial from 2008 they exposed 10 mice to aerosolized influenza A and aerosolized chlorine dioxide at (0.03 ppm) simultaneously for 15 minutes. A control group of 10 mice were exposed to only the aerosolized influenza A for 15 minutes. Sixteen days after exposure, none of the mice exposed to the chlorine dioxide influenza A group had died, but 7 out of 10 mice in the influenza only control group died. That is a 70% fatality for the mice that did not receive aerosolized chlorine dioxide. Did you catch that? Extremely low doses of chlorine dioxide protected 100% of those mice from influenza.
Moving past in vitro and in vivo trials, in a later post I will review the efficacy of chlorine dioxide in the treatment of infectious and other diseases in humans. There I will provide a compilation of all published human clinical trials and studies (which are artificially few due to the suppression of clinical research using chlorine dioxide.
A comprehensive list of all organisms it has been studied and shown efficacy against is beyond the scope of this post, however, know that in a 2010 study, concentrations ranging from 1 to 100 ppm inactivated ≥ 99.9% of the viruses with a 15 sec treatment. The antiviral activity of CD was approximately 10 times higher than that of sodium hypochlorite which is standard bleach.
NASA actually referred to chlorine dioxide as “A Universal Antidote” back in 1988 (p.118 from this Annual Report), where these statements appear:
- The special properties of the Alcidem formulation, which has been approved by U.S. regulatory authorities, enable it to destroy mold and fungus, as well as bacteria and viruses, with minimal harm to humans, animals or plants
- NERAC conducted a computer search of more than a dozen databases and uncovered scores of applications, among them treatment of viral, fungal and bacterial infections in animals; treatment of human skin diseases; disinfection and sterilization of medical facilities;
- The University of Connecticut Medical School is studying the effects of the Alcide compound on human wound healing and scar tissue suppression.
- At Israel’s Hebrew University Dental School, trials are in progress on a plaque reducing mouthwash and in England researchers are meeting success in human clinical trials of treating herpes and other sexually transmitted diseases.
I cannot over emphasize the importance of the above NASA document from 1988. In it, they admit that it treats a broad range of infections in animals, aids in wound healing (I have a lot on that later), and was having success in treating herpes and other STD’s. Never forget this when you read statements from regulatory agencies across the world where they repeatedly warn that it is a “toxic bleach,” “bleach like substance,” and is “dangerous for ingestion.” Absurd.
Also take note of the fact that NASA never refers to it again in such a positive way. The next mention by NASA was in 1991 when referring to its use in the space shuttle where they caution of the risk of developing hemolytic anemia and disturbing thyroid function (such risks are negligible to non-existent in clinical practice).
Therapeutic Mechanisms Of Action
- Anti-bacterial mechanisms: chlorine dioxide interacts intricately with sulfur-containing compounds that are abundantly found in various bacteria. This interaction disrupts the metabolic processes of these microorganisms, effectively inhibiting their reproduction and growth. Remarkably, at lower concentrations of 0.25 mg/L, CD can eradicate 99% of E. coli (15,000 cells/mL) within a mere 15 seconds.
- Anti-fungal mechanisms: causes significant damage to fungal cell membranes. This damage leads to the leakage of intracellular components such as potassium ions (K⁺) and adenosine triphosphate (ATP), suggesting that ClO₂ disrupts membrane integrity.
- Anti-viral mechanisms: ClO₂ inactivates viruses by oxidizing specific amino acids, such as cysteine, methionine, tyrosine, and tryptophan, in viral proteins. This oxidative modification leads to protein denaturation, impairing the virus’s ability to infect host cells. ClO₂ reacts with viral components, including proteins and genetic material. These reactions compromise the virus’s structural integrity and functionality, leading to its inactivation. In its gaseous state, ClO₂ can penetrate the outer shells of encapsulated viruses, leading to their inactivation.
In this post, Andreas Kalcker describes the “dual properties” of CDS:
It possesses the unique ability to effectively oxidize pathogens that exhibit an oxidation-reduction potential (ORP) lower than its own ORP of 0.95V. This means that it can target and neutralize various harmful microorganisms, including bacteria, viruses, and fungi, by disrupting their cellular processes and ultimately leading to their demise.
At the same time, CDS also functions as a powerful reducing agent, as it can interact with and reduce harmful free radicals that have higher ORPs—such as hydroxyl radicals (OH-) which possess an ORP of 2.8V. In this process, chlorine dioxide transforms these detrimental radicals into harmless water molecules. This dual functionality is particularly important in the context of therapeutic applications, as it allows CDS to both eliminate harmful agents while simultaneously protecting healthy cells from oxidative stress.
From this masterful review article in the University of Guadelajara journal on mechanisms of chlorine dioxide, they report even more broadly systemic therapeutic mechanisms:
- low concentrations of ClO2 can protect erythrocytes (red blood cells) from oxidative stress while inhibiting myeloperoxidase (MPO)-mediated excessive hypochlorous acid (HClO) production, thus reversing inflammatory responses and macrophage activation.
- increases the expression of heme-oxygenase (HO-1), protects cells from death caused by hydrogen peroxide (H2O2), enhances the expression and activities of antioxidant enzymes, such as superoxide dismutase, catalase and glutathione peroxidase, and contributes to the resolution of the inflammatory process.
- It promotes apoptosis (programmed cell death) in neutrophils, which helps resolve inflammation effectively
- It has demonstrated anti-inflammatory responses by inhibiting macrophage activation in humans, thus reducing inflammation
- Here it is important to review the different types and functions of macrophages (our immune system’s first line of defense against toxins and pathogens) :
Monocytes are bone marrow derived precursors of tissue macrophages that are critical effectors of wound healing, clearance of bacteria and cellular debris and induction and resolution of inflammation. Macrophages that are associated with classical inflammation are termed M1 and those cells produce factors such as TNF-α, IL-1 and other proinflammatory factors. Macrophages that are associated with reversal of inflammation and suppression of immune responses are termed M2. In the context of ALS pathogenesis, the M2 macrophage phenotype within the spinal cord is associated with normal function, whereas the appearance of new M1 type macrophages within the spinal cord is associated with disease progression.
These data suggest that systemic macrophage associated inflammation may play a significant role in ALS disease progression.“ In this study of a chlorine dioxide precursor in ALS, they report “these mechanisms of downregulation transform inflammatory monocytes/macrophages from a proinflammatory to a basal phagocytic (wound healing) state.”
I will cover the studies showing improved survival and function in ALS patients in a later post.
- taurine-chloramine is a product of activated neutrophils and represents the most relevant functional product formed under the influence of chlorine dioxide. This molecule activates nuclear factor erythroid 2 (Nrf2), (this transcription factor regulates the inducible expression of numerous genes for detoxifying and antioxidant enzymes), and inhibits production of pro-inflammatory cytokines.
- In a study of a different precursor, they report, “Of importance, a single dose of NP001 (a patented formulation of chlorite) caused a dose-dependent reduction in downregulation of CD16-expressing inflammatory macrophages in blood.”
- In this study, they found that the above WF10 (another patented formulation) exerts potent immune-modulatory effects through generating endogenous oxidative compounds such as taurine chloramine. Proliferation and IL-2 production of anti-CD3 stimulated PBMC were inhibited by WF10, as was the nuclear translocation of the transcription factor NFATc.
- In another study of the NP001 proprietary formulation of pH stabilized, purified chlorite, they found that in the presence of heme-associated iron, presumably from the nicotinamide adenine dinucleotide phosphate (NADPH) oxidase complex on the surface of phagocytic cells, it is converted from a prodrug through a hypochlorite intermediate, to an intracellular form of taurine chloramine (TauCl). TauCl is a long-lived effector molecule within macrophages that down-regulates NF-kB expression and inhibits production of pro-inflammatory cytokines in part through activation of heme oxygenase-1 (HO-1). A phase 1 controlled trial of NP001 in patients with ALS demonstrated the safety, tolerability, and dose dependent down-regulation of monocyte activation.
More therapeutic mechanisms:
Taken from this Andreas Kalcker substack post, he describes the effects of chlorine dioxide solution (CDS) using venous blood gas analysis:
- The blood pH became more alkaline, indicating a reduction in acidity and an increase in basicity.
- Blood oxygen levels increased, suggesting enhanced oxygenation throughout the body.
- The concentration of carbon dioxide (CO₂) in blood decreased, implying effective CO₂ elimination via respiration.
- There was an observable improvement in acid-base balance, particularly in base deficit, reflecting better pH regulation within the body, essentially reducing metabolic acidity, frequently a fundamental factor in numerous modern diseases
- Blood glucose levels normalized, with reductions in hyperglycemia noted in other cases.
- A significant decrease in blood lactic acid levels was observed, indicating improved removal of metabolic waste products.
Based on the above and considering the molecular composition of chlorine dioxide (two atoms of oxygen), Kalker argues in his mechanisms of action post here (where I paraphrase for brevity:
“chlorine dioxide transports oxygen to all parts of the body where water is present. The bound oxygen dissociates in the presence of excess protons in areas of disease (like spike protein). The released oxygen optimizes the saturation of hemoglobin in the red blood cell and thus improves oxygen delivery to the most acidic cells and their compromised mitochondria first, while the chlorine ion (not chloride) eliminates pathogens or acidic toxins and restores pH balance. This improvement in cellular oxygenation is thought to be yet another positive therapeutic mechanism for reversing disease.
Images depicting the effects of CDS on blood on a Nikon Phase contrast Microscope:

Effects of CDS in Human Blood under phase contrast microscope
In these phase contrast microscopy images above, the impact of CDS on small red blood cells is clearly visible. Initially, the cells were highly agglutinated and oxygen-deprived. Following the infusion of CDS at a maximum concentration of 3000 ppm from the left side, immediate signs of oxygenation can be observed. After a mere 12 minutes, all blood cells exhibit optimal oxygenation levels.
**As a pulmonologist, I don’t know how you can “see” improved oxygenation, although it can be inferred by the dramatic increase in the exposed surface area of each blood cell as they de-aggregate.
Overall, studies and treatment experiences reveal that treatment with chlorine dioxide:
- is broadly antimicrobial against nearly all infectious pathogens
- reduces inflammation
- prevents scarring
- aids in wound healing
- is non-toxic when orally ingested (in appropriate concentrations)
- reduces oral plaque
- treats oral atrophic candidiasis
- is a potent deodorizer
- has in-vitro anti-cancer cell effects, stimulates an in-vivo anti-cancer cell immune response and is also effective when injected intra-tumorally, or via a combination of oral, enema, and IV administration.
This combination of properties is not found in any other compound. The therapeutic uses for chlorine dioxide are endless. And therein lies the problem. Stay tuned for my upcoming post which compiles the studies and trials in a diverse set of human diseases.
** Please know that I am not recommending that anyone use chlorine dioxide orally given it is not FDA approved for oral ingestion in any medical condition, nor has it been approved by any foreign regulatory agency, nor is it classified as a food supplement. What I am trying to do is amass the critical information needed to petition the “new” FDA (and other regulatory agencies worldwide) to remove their restriction on performing human subjects research with orally ingested chlorine dioxide.
A Comprehensive Guide to Treating Pink Eye
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2025/01/15/pink-eye-treatment.aspx
Analysis by Dr. Joseph Mercola January 15, 2025

Story at-a-glance
- Viral conjunctivitis (“pink eye”) is highly contagious and typically caused by adenovirus, presenting with red, irritated, crusty, and watery eyes
- Bacterial pink eye produces thick yellow-green discharge and typically affects one eye initially, while viral cases often accompany cold symptoms like sore throat and runny nose
- Nebulized hydrogen peroxide diluted to 0.1% concentration and applied via face mask over affected eye(s) can rapidly eliminate viral pink eye symptoms
- Essential preventive measures include proper hand hygiene, avoiding eye touching, not sharing personal items, and maintaining good immune health through sleep, stress management, and exercise
- Medical attention is needed if symptoms include intense eye pain, increased light sensitivity, vision changes, or if the patient is immunocompromised, as complications like keratitis can lead to vision loss
Have you ever woken up one morning to find your eyes are red, irritated, crusty and watering excessively? This common scenario describes viral conjunctivitis, often referred to as “pink eye.”
While it might seem like a minor inconvenience, viral conjunctivitis can significantly impact your daily life and eye health. Unlike bacterial or allergic conjunctivitis, viral conjunctivitis is caused by viruses, most commonly the adenovirus. These viruses often accompany other viral infections like the common cold or flu.
Viral conjunctivitis is highly contagious and can spread rapidly, especially in communal settings like schools and workplaces.
Recognizing the Key Differences Between Allergic, Bacterial and Viral Conjunctivitis
Understanding the differences between viral, bacterial, and allergic conjunctivitis is crucial for effective treatment and recovery.
• Allergic conjunctivitis stems from allergens like pollen or pet dander, leading to itchy, watery eyes.
• Bacterial conjunctivitis is caused by bacteria such as Staphylococcus aureus, Streptococcus pneumoniae, and Haemophilus influenzae, typically resulting in thick, yellow-green discharge that can cause the eyelids to stick together, especially after sleep. These bacteria can enter the eye through direct contact with contaminated hands, surfaces, or respiratory droplets.
Redness may be more pronounced in one eye initially but can spread if not treated promptly. Noticeable swelling or puffy eyelids are more common in bacterial cases. Unlike viral conjunctivitis, bacterial conjunctivitis typically does not present with systemic symptoms like a runny nose or sore throat, which can help in distinguishing it from its viral counterpart.
Bacterial conjunctivitis often exhibits a faster onset of severe symptoms, escalating quickly within a day or two and becoming more severe if left untreated. Without appropriate treatment, bacterial conjunctivitis can spread to both eyes and lead to more serious eye infections, underscoring the importance of timely medical intervention.
• Viral conjunctivitis is an infection of the conjunctiva, the thin, clear tissue that lines the inside of your eyelid and covers the white part of your eye. Common symptoms include noticeable redness in the white of the eye or inner eyelid, excessive watery discharge from the eyes, a persistent itching or burning sensation that makes blinking uncomfortable, and a watery or mucus-like discharge that may form a crust, especially upon waking.
Additionally, viral conjunctivitis may include symptoms such as a runny nose, sore throat, or fever, indicating an underlying viral infection. Patients may also experience a persistent itching or burning sensation, though it is generally less intense than what is observed in allergic conjunctivitis.
Viral conjunctivitis spreads through direct contact with infected secretions, contaminated surfaces, or respiratory droplets from an infected person’s cough or sneeze. Sharing personal items like towels, makeup, or contact lenses can also facilitate the transmission of the virus.
Several factors increase the risk of contracting viral conjunctivitis, including living in close quarters with someone who is infected, having a weakened immune system, and poor hygiene, such as infrequent handwashing or touching the eyes with unwashed hands.
Viral conjunctivitis symptoms can persist for one to two weeks, gradually improving as the body fights off the virus. Most cases resolve without the need for antibiotics, relying on your body’s immune response for recovery.
Conventional Medical Treatments
Conventional treatments for viral conjunctivitis focus primarily on relieving symptoms. Supportive care, such as artificial tears and lubricating eye drops, can soothe irritation and reduce redness.
Applying a clean, cold cloth over closed eyes can alleviate discomfort and swelling. In severe cases, especially those caused by the herpes simplex virus, antiviral eye drops or ointments may be prescribed.
However, while conventional treatments can ease symptoms, they don’t directly target the underlying viral infection. Additionally, the misuse of antibiotics for viral conjunctivitis can contribute to antibiotic resistance and may lead to unnecessary side effects. Accurate diagnosis is also essential to avoid inappropriate treatments.

Save This Article for Later – Get the PDF Now
Natural Remedies Work Far Better
Maintaining impeccable hygiene is your first line of defense against viral conjunctivitis. Washing your hands thoroughly with soap and water, especially before touching your face or eyes, is essential. That said, excessive handwashing is counterproductive and can increase your risk of infections by damaging the skin on your hands.
Avoid touching or rubbing your eyes to prevent further irritation and the spread of the virus. Additionally, avoid sharing personal items like towels, pillows, or makeup to minimize transmission risks.
A nutrient-rich diet supports overall eye health and immune function. Vitamins A, C, and E are antioxidants that protect eye tissues and support immune health. Incorporating foods like carrots, citrus fruits, and leafy greens into your meals can provide these essential nutrients. Omega-3 fats, found in small cold-water fatty fish, reduce inflammation and promote eye health.
Staying hydrated by drinking plenty of water also maintains optimal eye moisture and supports your body’s natural defenses. Other lifestyle strategies that support your immune function include:
• Sleep — Aim for 7 to 9 hours of quality sleep each night to allow your body to repair and strengthen its defenses.
• Stress relief — Chronic stress can weaken the immune system, so practicing relaxation techniques like meditation, deep breathing, or yoga is beneficial.
• Exercise — Engaging in moderate physical activity boosts circulation and supports immune health.
Nebulized Hydrogen Peroxide Can Eliminate Pink Eye in 30 Minutes
One of the most effective ways to rapidly eradicate viral infections is with nebulized peroxide, and this works for pink eye as well. I recently treated myself this way, after I woke up with viral conjunctivitis in one eye, and 30 minutes after treatment, my symptoms were all gone.
As for respiratory infections, all you need is a nebulizer that emits a fine mist with properly diluted food grade hydrogen peroxide. The only difference is that you place the face mask over the affected eye(s) instead of your mouth and nose.
Typically, food grade peroxide comes in concentrations of 3% or 12%, which must be diluted down to 0.1%, as described in the chart below.
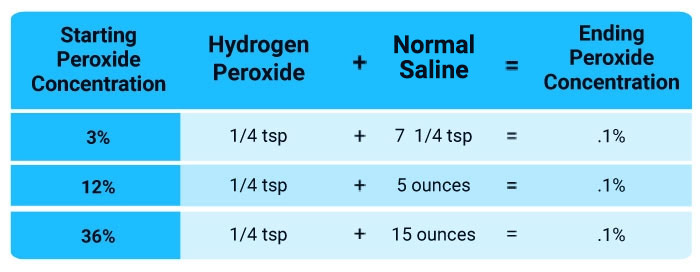
Hydrogen peroxide (H2O2) consists of a water molecule (H2O) with an extra oxygen atom, and it is the additional oxygen atom that allows it to inactivate viral pathogens.
Some of your immune cells actually produce hydrogen peroxide to destroy pathogens. By killing the infected cell, viral reproduction is stopped. So, hydrogen peroxide therapy is in essence only aiding your immune cells to perform their natural function more effectively.
When to Seek Medical Attention
While viral conjunctivitis is generally self-limiting, certain situations warrant professional medical evaluation. Persistent or intense eye pain may indicate a more serious condition that requires immediate attention.
Increased sensitivity to light can be a sign of corneal involvement or other complications that need prompt assessment by an eye care professional. Any changes in vision should also be taken seriously and evaluated to rule out more severe issues.
Viral conjunctivitis can lead to complications such as keratitis, which is inflammation of the cornea that can result in scarring and vision loss if left untreated. Bacterial superinfection can also occur, necessitating antibiotic treatment.
Special considerations should be made for infants, the elderly, and those with compromised immune systems, as these groups are more susceptible to severe infections and complications.
Dispelling Myths About Viral Conjunctivitis
It’s important to clarify common misconceptions surrounding pink eye to promote accurate understanding and effective management.
One common misconception is that all pink eye is highly contagious. While viral conjunctivitis is indeed contagious, bacterial and allergic types are not necessarily so. Understanding the specific type helps in managing transmission risks effectively.
Another myth is that antibiotics are effective for viral conjunctivitis. Antibiotics only work against bacterial infections and are ineffective against viral causes. Misusing antibiotics can contribute to antibiotic resistance and other side effects, emphasizing the importance of accurate diagnosis.
Additionally, the belief that viral conjunctivitis always requires medical treatment is not entirely accurate. Most cases resolve on their own with supportive care. However, severe or complicated cases may need medical intervention, underscoring the importance of recognizing when professional help is necessary.
Supporting Overall Eye Health
Regular eye exams, even if you don’t experience symptoms, can detect issues early and keep your eyes functioning at their best. Annual check-ups are recommended, especially if you wear contact lenses or have a history of eye conditions.
Protective measures are also important. Wearing protective glasses or goggles during activities that pose a risk to your eyes, such as sports or certain work environments, will help prevent injuries and infections.
Maintaining a healthy lifestyle also contributes to eye health. Avoiding smoking reduces the risk of eye diseases like cataracts and macular degeneration. Managing chronic conditions such as diabetes and hypertension is also essential, as these conditions can adversely affect eye health.
So, in closing, viral conjunctivitis, while common and often self-limiting, can cause significant discomfort and inconvenience. Understanding its causes, recognizing symptoms, and using natural remedies such as nebulized hydrogen peroxide can empower you to manage and prevent this condition effectively.
Embracing a holistic approach — focusing on hygiene, nutrition, immune support, and natural remedies — will enhance your eye health and overall well-being over the long term.
Guard against bacteria and fungi with THIS natural defender
Reproduced from original article:
https://www.naturalhealth365.com/guard-against-bacteria-and-fungi-with-this-natural-defender.html
by: June 12, 2024
 (NaturalHealth365) As you know, Western medicine relies heavily on antibiotics to treat infections – and sometimes, these drugs are truly needed. But the rise of antibiotic-resistant “superbugs” – along with the unwanted side effects that can accompany antibiotic use – has triggered an urgent search for naturally sourced substances, oregano oil, to kill pathogens safely and effectively.
(NaturalHealth365) As you know, Western medicine relies heavily on antibiotics to treat infections – and sometimes, these drugs are truly needed. But the rise of antibiotic-resistant “superbugs” – along with the unwanted side effects that can accompany antibiotic use – has triggered an urgent search for naturally sourced substances, oregano oil, to kill pathogens safely and effectively.
In fact, recently published research reveals the potential of a familiar Mediterranean cooking herb to do just that, and the results are stunning.
Oregano oil has potent effects against Candida albicans
A member of the mint family, oregano is scientifically known as origanum vulgare L. The name “oregano” derives from the Greek words for “mountain” and “joy” – and oregano certainly seems to be bringing joy to researchers when it comes to its surprising antimicrobial properties.
In a study conducted at Georgetown University Medical Center and published in Molecular and Cellular Biology, the research team investigated the ability of oregano essential oil to kill Candida albicans. This fungal yeast overgrowth can cause joint pain, exhaustion, and digestive problems.
They found amazing results: at concentrations of .25 mg/ml, wild oregano oil – a blend known as P73 – completely inhibited both the germination and the mycelial growth of C. albicans in cultures.
The team credited the oil with “potent’ antifungal effects against C. albicans.
Defend against dangerous bacteria and viruses
In a 2012 study, researchers found that oregano essential oil inhibited the growth of 20 different clinical bacterial strains of E. coli – which can cause severe gastrointestinal problems, anemia, and even kidney failure – and 20 strains of P. aeruginosa, which can cause ear infections, skin rashes, and pneumonia.
The encouraging results led researchers to call for further study on oregano oil as an alternative antibacterial remedy – and to explore its use as an “effective means for the prevention of antibiotic-resistant bacteria.”
And there’s more.
Additional studies have shown that oregano oil kills at least 30 different strains of disease-causing bacteria, including staphylococcus aureus, the leading cause of skin and soft tissue infections, and coronavirus, a primary cause of the common cold, pneumonia, and other respiratory infections.
In addition, oil of oregano kills the H. pylori bacterium – a contributory factor in 90 percent of all duodenal ulcers and 80 percent of all gastric ulcers.
What makes this all-natural oil so potent?
Oregano’s two most formidable weapons are a pair of volatile oils, thymol and carvacrol. Carvacrol has also been studied for its therapeutic effects, and a 2016 study published in the European Review for Medical and Pharmacological Sciences showed that carvacrol from oregano oil protected against methotrexate toxicity.
Other constituents of oregano include various flavonoids, essential vitamins, and minerals, including iron, manganese, vitamin E, tryptophan, and omega-3 fatty acids. Oregano also contains ursolic acid, a powerful antioxidant and antibacterial agent.
Even MRSA is no match for this potent essential oil
Did you know that the World Health Organization (WHO) has classified the advent of “superbugs” as a global public health crisis? Currently, methicillin-resistant staphylococcus aureus – or MRSA – strikes 80,000 people and claims over 11,000 lives worldwide every year. Just don’t expect any organization – like WHO – to tell you the health benefits of a substance like, oregano oil.
By the way, the news about oregano oil just keeps getting better. A team of British and Indian researchers reports that the essential oil of Himalayan oregano – simply, origanum vulgare, which happens to grow in the Himalayas – is effective against the MRSA pathogen.
According to researcher Professor Vyv Salisbury, the essential oil kills MRSA at a dilution of 1 to 1,000. The oil kills MRSA both as a liquid and a vapor, and its antimicrobial ability is undiminished by heating in boiling water.
Plans are underway to develop an oregano-based soap for use in hospitals, both for washing hands and disinfecting surfaces.
How should I take this powerful essential oil?
P73 oil of oregano is available in capsule form.
Natural healthcare providers will often advise the use of oregano essential oil for colds, flu, sinusitis, and other respiratory illnesses, as well as for candida and yeast infections.
It can also be used for duodenal and gastric ulcers – in conjunction with other medications that target H. pylori – and, when mixed with coconut oil, can be used topically for athletes’ foot and ringworm.
Because oregano oil is so potent, you should only use it under the guidance of your trusted holistic physician, who can advise you on the correct amount. Some experts say oil of oregano should be diluted with water or mixed with coconut oil and not taken internally for more than two weeks.
Because oregano oil is such an effective antibacterial agent, long-term use can deplete levels of friendly gut bacteria. So it’s wise to make sure you consume sufficient amounts of probiotic foods – such as live-cultured yogurt, miso soup, or raw sauerkraut – along with prebiotic foods such as organic garlic, onion, and asparagus.
Sources for this article include:
NIH.gov
NIH.gov
NIH.gov
Medicalnewstoday.com
Medicalnewstoday.com
The Health Benefits of Getting Dirty
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2024/06/03/health-benefits-of-getting-dirty.aspx
Analysis by Dr. Joseph Mercola June 03, 2024

STORY AT-A-GLANCE
- Evidence demonstrates that getting dirty is one key to a healthy immune system, a lower rate of allergies and asthma and a better mood, as it can help seed your skin and gut microbiome with beneficial microbes
- The Hygiene Hypothesis proposes that without exposure to bacteria you are at higher risk of illness. Conversely, the Farm Effect proposes that children and adults who are routinely exposed to dirt and animals have a lower risk of the same
- Someday, today’s population may be known as the indoor generation as most people spend up to 90% of their time inside
- Gardening reduces stress and exposes you to soil-based Mycobacterium vaccae, which animal and clinical studies have demonstrated has anti-inflammatory properties that can affect mood
- Embracing the outdoors may help reduce your seasonal allergy reactions. Consider taking probiotics, avoiding antibacterial soap, eating organic and fermented foods, and getting your hands dirty in your garden
One key to a healthy immune system, a lower rate of allergies and a better mood might be getting dirty. But not just any dirt. This isn’t the dust in your house or grease from the garage. The dirt I’m talking about is in the garden, or your pots if you live in an apartment.
According to the Asthma and Allergy Foundation of America,1 roughly 1 in 3 adults and 1 in 4 children in the U.S. have seasonal allergies, eczema or a food allergy. In 2021, 81 million people were diagnosed with seasonal allergic rhinitis, which was 26% of adults and 19% of children. Seasonal allergies cause 3.1 million missed workdays and cost $8 billion annually.2 In other words, it’s nothing to sneeze at.
Your gut microbiome, which is affected by your exposure to dirt, also influences your mood, including depression and anxiety. There is a crucial relationship between anxiety and depression.3 In 2020 and 2021, researchers estimated the prevalence of anxiety from 26.9% to 31.9% and the prevalence of depression from 28% to 33.7%.4 Those percentages represent a large part of the U.S. population.
The first line of treatments for seasonal allergies, anxiety and depression are medications, many of which come with a long line of side effects. The good news? There is strong data to suggest that by carefully cultivating your gut microbiome you may influence your risk and severity of allergies and mood disorders.
Why a Little Bit of Dirt May Be Healthy for You
It’s called the Farm Effect or the Hygiene Hypothesis. The basic idea is that the more you’re exposed to soil and dirt, the more diverse your gut microbiome and the stronger your immune system, which affects many physiological processes.
In 1989, David Strachan a professor of epidemiology at the University of London/St George’s Hospital5 published a paper6 proposing that children who were exposed to more germs were less susceptible to developing disease and illness as they grow. He found differences between children who had more and fewer siblings. This was dubbed the “Hygiene Hypothesis,” which was then framed as “the Old Friends” or “microbiota hypothesis.”7
A 2012 paper8 found that microbial diversity plays a central role in protective effects against asthma and allergies. The researchers found individuals exposed to cows, straw and drinking unprocessed, raw milk just three times experienced protective effects from asthma but not atopy (eczema and allergic rhinitis).
This was dubbed the “Farm Effect,” “one of the most compelling observations to arise from investigations of the microbiome in asthma development, and it is one of the key phenomena that has maintained the relevance of the hygiene hypothesis.”9
Exposure to microbes when you’re young can lead to a much lower risk of asthma and allergic inflammation when you’re older. Researchers have proposed exposure to animal-associated microbes is key, yet analysis of the published data finds potential gaps and questions the specific exposures that offer the best protective effect.
A 2016 study10 in The New England Journal of Medicine identified some significant differences. The researchers analyzed the rates of asthma and allergies among Amish communities,11 including the Hutterites, who are a group living largely in Canada and the northwest U.S. While both communities make their livelihood from farming, Amish families use traditional methods, including livestock power tools while Hutterites use modern farm machinery.
The researchers found that only 10% of Amish school children were diagnosed with asthma and allergies while up to 30% of Hutterite children experienced those conditions. The researchers concluded that the dust from the farm fields might protect the Amish children while being sheltered from the exposure might increase the vulnerability of Hutterite children.
Proper Hygiene Has Its Place
Regular hand washing became a strong focus of public health agencies during and after 2020 to remove germs, avoid illness and prevent the spread of germs to others.12 The importance of hand washing to prevent the spread of infection became a worldwide focus in 2008 during the first Global Hand Washing Day.13
Many parents spend a good deal of time teaching young children the importance of taking baths, washing their hands before meals or staying as clean and germ-free as possible. Is this counterintuitive to the Farm Effect, Hygiene Hypothesis and multiple studies demonstrating that many of our kids may have become too clean for their own good?
No, it isn’t. Exposure to common viruses is not what seeds your gut microbiome with beneficial bacteria. Hand washing to reduce the spread of viral infections is necessary, but digging into a handful of soil or hiking through the woods offers exposure to different live cultures.
Save This Article for Later – Get the PDF Now
Being Out in Nature Helps Seed Your Microbiome
Someday, today’s population might be known as the indoor generation. A report on a survey from window manufacturing company VELUX found nearly 1 in 4 Americans spend their entire day indoors without ever going outside.14
On average, the 16,000 people from 14 countries who were surveyed believed they spent 18% of their day inside, but the actual amount was 90%. Peter Foldbjerg, head of daylight energy and indoor climate at VELUX, said in a press release:
“With the pressures of modern life, we are all now firmly a part of the Indoor Generation and we need to understand the implications on our health and wellbeing of life indoors, as well as outdoors, when it comes to polluted air.
We are a 24/7 society and this has disconnected us from the natural rhythms of nature — our circadian rhythm, a neurophysiological term for the 24-hour body clock that anticipates and adapts our physiology to the different phases of the day, sleep and wake cycle. All of this impacts our sleep quality and general health.”
So, while the first step is to step outside, the second step might be to get your hands in the dirt. Scientists have discovered the broad range of benefits that microbes play on mental and physical health. Christopher Lowry, professor of integrative physiology at the University of Boulder Colorado told The New York Times that when we are outside, “we’re breathing in a tremendous amount of microbial diversity.”15
A study from Finland revealed that children who went to nature-oriented daycare centers experienced greater biodiversity in their skin microbiome and gut bacterial community. The researchers found correlations between the gut microbiota and their immunological systems concluding that the results:16
“… support the biodiversity hypothesis and the concept that low biodiversity in the modern living environment may lead to an uneducated immune system and consequently increase the prevalence of immune-mediated diseases.”
Anti-inflammatory Fat in Soil-Dwelling Bacterium May Affect Mood
Soil exposure may not only help allergies and asthma, but it could affect your mood. In a 2004 paper17 published in the Annals of Oncology, physicians reported the effect of injecting SRL172, (killed Mycobacterium vaccae) alongside chemotherapy to treat non-small cell lung cancer.
The researchers had hypothesized this may help the body fight cancer based on previous studies where the suspension was used in individuals with drug-resistant pulmonary tuberculosis18 and to boost immune system response.19
However, the data showed there was no difference between the control group who did not receive SRL172 and the intervention group in overall survival, which was the primary endpoint of the study.
The researchers found that patients who received SRL172 experienced improved quality of life in the time they had left. This was a unique demonstration of the influence the bacterium had over mood in a group of individuals who were facing a challenging health condition.
In 2007,20 Lowry injected heat-killed or M. vaccae into mice and exposed them to stress tests. The animals that received the bacteria demonstrated less stress during the tests. A later research group21 fed mice the bacterium and found they ran mazes twice as fast and enjoyed doing it. The researchers theorized it had something to do with the effect on the immune system.
In 2010, Dorothy Matthews of the Sage Colleges, presented her results at the annual American Society for Microbiology meeting. They found the bacteria appeared to stimulate the hippocampus, which is responsible for spatial memory and changed the mice’s mood as they demonstrated less anxiety-related behavior.
“It just shows that we evolved with dirt as hunter-gatherers,” she said. “So, turn off your TV and go work in your garden, or walk in the woods.”22
Lowry continued studying Mycobacterium vaccae and in 2019 he published information on anti-inflammatory fat found in the bacterium that might explain the effect it has on mood and stress.23 The anti-inflammatory fat — 10(Z)-hexadecenoic acid — appear to inhibit inflammation in immune cells. The research supports the Farm Effect and brings researchers closer identifying how it could help reduce stress and anxiety for those in high-stress jobs.
Embracing the Outdoors May Reduce Your Seasonal Allergy Reactions
Thankfully, you don’t have to live on a farm to experience the Farm Effect. While taking probiotics and prebiotics can help reseed your gut microbiome and affect your overall health, several more steps can prevent damage and help improve your microbiome diversity.
| Stop using antibacterial soap and detergents — Regular soap and water can clean your hands, and there is no evidence that antibacterial soap offers more benefits.24 |
| Clean up your diet — Choose organically grown foods and eliminate products grown with genetically modified seeds or sprayed with pesticides and insecticides as these destroy your gut bacteria. |
| Eat fermented foods — Fermented vegetables are inexpensive and easy to make at home and provide a host of health benefits, including seeding your gut microbiome. |
| Go gardening — No matter where you live you can garden. Even in an apartment, you can grow plants in pots and get your hands dirty. Just remember to leave the gardening gloves for when you’re pruning plants with thorns and use your bare hands for planting. |
| Get dirty — Children love getting dirty, and adults may want to take a page from their playbook. Think about playing in the dirt or mud, making mud pies, bug hotels, fairy gardens or even mud art. Take up a mud sport like mud runs, mountain biking or hiking. The idea is to just get dirty. “I think we underestimate how much exposure we get from simply being outside,” Lowry said.25 |
| Not all dirt is good dirt — Steer clear of dirt in polluted areas that contain harmful contaminants and can be unhealthy for children and adults. Don’t use chemical weed killer or glyphosate and choose the best soil possible for your pots and raised gardens so you enjoy the same benefits as your plants. |
- 1 Asthma and Allergy Foundation of America, Allergy Facts, Green bar #2 & #7
- 2 Allergy and Asthma Network, Allergy Statistics in the U.S.
- 3 American Journal of Psychiatry, May 1, 2020, Abstract
- 4 Journal of Family Medicine and Primary Care, 2023; 12(6)
- 5 St. George’s University of London, Professor David Strachan
- 6 BMJ, 1989; 299(6710)
- 7 Archives of Medical Research, 2017;48(8)
- 8 Current Opinion in Allergy and Clinical Immunology, 2012; 12(5)
- 9 The Journal of Allergy and Clinical Immunology, 2021; 148(1)
- 10 The New England Journal of Medicine, 2016; 375
- 11 Stat News, August 3, 2016
- 12 Centers for Disease Control and Prevention, May 4, 2023
- 13 Global Hand Washing Partnership, About Global Handwashing Day
- 14 PR Newswire, May 15, 2018
- 15, 25 The New York Times, April 17, 2024
- 16 Science Advances, 2020;6(42)
- 17 Annals of Oncology 2004; 15(6)
- 18 Respiratory Medicine, 2001; 95(6)
- 19 Immunology, 2001; 102(2)
- 20 Neuroscience, 2007; 146
- 21, 22 New Scientist, May 27, 2010
- 23 Neuroscience News, May 29, 2019
- 24 Centers for Disease Control and Prevention, November 4, 2022, Soap (Archived)
Why Does Science Still Ignore Vitamin C?
Reproduced from original OMNS article (OrthoMolecular News Service):
http://orthomolecular.org/
Subscribe to the free Orthomolecular Newsletter: http://orthomolecular.org/subscribe.html
Go to the OMNS Archive: http://orthomolecular.org/resources/omns/index.shtml
Orthomolecular Medicine News Service, May 18, 2022
From colds to Covid, ascorbate has long been marginalized
by Pim Christiaans
OMNS (May 18, 2022) For more than 20 years, Dr. Harri Hemilä, biochemist, physician and epidemiologist, has been analyzing research conducted with vitamin C. In 2017, ORTHO magazine had an interview with him. [1] At that time, the interest in vitamin C was mainly about the common cold. Now it also concerns another virus infection, Covid-19. Has anything changed since then? The near-total lack of interest within medical science for vitamin C still exists. And apparently, medical professors don’t give a damn about the vitamin, as if it were a career killer.
Since 2002, Hemilä has considered it his professional duty to analyze studies conducted on vitamin C and to publish the analyses. What is the common thread after more than a hundred scientific publications, of which twelve were published in the years 2020 and 2021, and three in 2022? Well, one of these three reveals that common thread. In a review article of 27 pages in the open access magazine Life, [2] Hemilä unfolds his experiences and explains them in a long telephone conversation with ORTHO. The title of the article speaks volumes: “Bias against Vitamin C in Mainstream Medicine: Examples from Trials of Vitamin C for Infections.” Remarkable. It turns out that prejudices (“bias”) are a major common thread in the medical scientific world.
Thousand versus half a million
In the article, Hemilä shows, among other things, that the authors of the COVID-A to Z Study wrongly conclude that vitamin C is ineffective against Covid-19, because the data they rely on incorrectly show otherwise. [3] This will be discussed in more detail below.
Hemilä is pleased that Life has published his extensive article on the prejudice against vitamin C for everyone to read. [2] However, he is under no illusions about its impact: “According to the counter on Life’s website, more than a thousand people have read my article. The COVID-A to Z Study on JAMA’s website also has a counter. And it was at half a million the last time I looked.”
In the Life article, Hemilä refers to articles by scientists who note that since the beginning of the last century, doctors and medical scientists have been writing about and discussing nutritional supplements with disdain. According to these researchers, over-the-counter vitamin pills undermined the authority of doctors, because they allowed the patient to self-treat. Moreover, it was not possible to patent nutrients, so there was little to gain for the pharmaceutical industry. And in the second half of the twentieth century, the discovery of patentable antibiotics overshadowed the promising effects of vitamin C against infectious diseases.
It was not until the end of the 1960s that there was renewed interest in the vitamin when Linus Pauling got involved. This led to a series of relatively large studies that, according to Hemilä, supported the effectiveness of vitamin C. Nevertheless, scientific interest in the vitamin fell again in the late 1970s. Hemilä points to the so-called “Karlowski Study” as the main cause, along with two other articles from 1975.
Start of the problem
In 1975, five years after the publication of Linus Pauling’s book Vitamin C and the Common Cold, the scientific journal JAMA published the results of the Karlowski Study, a double-blind randomized placebo-controlled trial of vitamin C. [4] Although colds in the group of subjects who took 6 grams of vitamin C were 17% shorter, the authors attribute this outcome entirely to a placebo effect. Hemilä did not agree with this, and in 1996 subjected the data to a thorough re-analysis. [5] Astonished, he concluded that the data in fact do show a real, physiological effect of vitamin C and that the placebo explanation is incorrect. He caught the authors making all kinds of mistakes. For example, 42% of the recorded colds were apparently omitted from the subgroup analysis without further explanation – an unforgiveable sin within the statistics. The data indicate a dose-response effect: the tested dose of 6 grams per day is twice as effective as the tested dose of 3 grams per day. Hemilä calculates that if you draw the line, a study with 12 grams of vitamin C would have been the obvious choice. Such a study, however, never materialized, partly due to the discouraging placebo explanation of the Karlowski Study.
He compares the Karlowski-Study to a zombie: “Although liquidated long ago, it refuses to disappear into the grave and continues to leave a trail of destruction through scientific literature.” Hemilä’s skilful disassembly of the Karlowski Study has never been disproved, but nevertheless has had little impact. According to him, this study has remained by far the most influential study on vitamin C and the common cold. The vitamin C skeptics couldn’t have it any better. There is a good chance that if a skeptical scientist mentions evidence on vitamin C, he will refer to this study.
Recent studies ignore evidence
Even now, according to Hemilä, studies are published with negative conclusions in their summaries, while the data on which they are based imply a very different conclusion. A good example of this is the ‘CITRIS-ALI study’ that was published in JAMA in 2019. [6]
In that study, participants were 167 patients in the ICU with sepsis and acute respiratory distress syndrome (ARDS). They received intravenous vitamin C (50 mg/kg body weight every 6 hours) or a placebo for four days. The researchers conclude: “A 96-hour infusion of vitamin C showed no significant improvement in organ dysfunction scores, nor did it alter markers of inflammation and vascular damage, compared to placebo.” but did not mention a major result: a strong decrease in mortality. Hemilä checked this and explained that during the first four days (when the vitamin C was administered) the mortality in the vitamin C group decreased by 81%. “The main clinically relevant result of the CITRIS-ALI trial was mortality and the measurement of a dozen biomarkers should not distract from that,” said Hemilä.
A second study
As a second example, Hemilä provided the previously mentioned COVID-A to Z-Study, which was published in JAMA Network Open in 2021. [3] The aim of that study was to evaluate the effect of 8 grams per day of vitamin C in 520 ambulatory Covid-19 patients. However, the study was terminated prematurely due to the slow influx of patients. This slowness led, as the researchers had mentioned, to a state of “futility.” [3] Therefore, in this aborted study, the number of patients remained at 214.
But Hemilä explained that this premature stopping was unjustified, because the effects of vitamin C were actually greater than the researchers had anticipated. [2] The researchers had expected a 1.0 day reduction in the duration of Covid-19, but they found a reduction of 1.2 days. Hemilä calculated that the recovery percentage in the vitamin C group was 70% greater than in the control group. None of this was reflected in the abstract of the article. The researchers, in turn, concluded that vitamin C did not significantly reduce the duration of symptoms.
How can this difference between the facts found and the conclusions of the research be explained? Hemilä does not need to look far: one of the authors of the COVID-A to Z-Study declared in the “Conflict of Interest” statement that she has carried out paid consultancy work for Gilead Sciences.” [3] This pharmaceutical company is the producer of Remdesivir, the first virus-inhibiting drug that was approved by the FDA for the treatment of Covid-19. Hemilä writes in his Life article: “What motivation does such a researcher have to find out whether a very cheap nutrient is actually effective against Covid-19 when an expensive drug available is available from a company for which she is a consultant?”
Timing purely coincidental
In February 2020, a team led by Harri Hemilä published a meta-analysis in the Journal of Intensive Care on the effect of vitamin C on the duration of artificial respiration given to ICU patients. [7] The timing was purely coincidental, but could not be better: the SARS-CoV-2 virus had only just started to spread from Wuhan and would cause death and destruction in the rest of the world in the months that followed. Hospitals’ intensive care units everywhere were overloaded by Covid-19 victims, some of whom had to be on artificial ventilation for an unusually long time. The article’s analysis seemed to imply a benefit from treatment with vitamin C. Hemilä and colleagues had collected data from eight studies involving a total of 685 patients who had ended up in ICU for a variety of reasons. Their calculations indicated that vitamin C had shortened the duration of artificial respiration by an average of 14%. In the most critically ill patients who had been on the ventilator the longest, vitamin C had actually reduced the duration by 25%.
More about vitamin C and Covid-19
The big question now is whether lives would have been saved if the vitamin had been given as standard to all Covid-19 patients in the ICU from the start of the pandemic as a precaution? Very likely, but we’ll never know. In any case, Hemilä’s hopeful article received little attention. The field has not rushed to start the bigger and better research studies called for in the last paragraphs.
In a telephone interview, Hemilä reacted resignedly to this finding: “It is a very big step to add vitamin C to the treatment protocol for Covid patients in ICUs. Based on our publication, it is too early for that. The studies we had to rely on were small and therefore of poor quality. However, there is very strong evidence for a biological effect of vitamin C, which justifies better and larger studies. In the meantime, you could assuredly give it to patients — because vitamin C is cheap, and safe even in doses of tens of grams administered orally or intravenously. This is again confirmed by a 2010 review of vitamin C researchers, including the first and last authors of researchers from the most respected institute in the US, the National Institutes of Health (NIH). [8]
Two quotes from Harri Hemilä:
Hemilä is not an uncritical apologist for Linus Pauling’s views:
“Pauling had a point, but he was too optimistic about vitamin C,” he says. “Unlike Pauling, I don’t think that an ordinary, healthy person would benefit from taking more than 500 mg of vitamin C per day. For the elderly, he recommended something like 10 grams of vitamin C per day, and I see no justification for that. But if people are sick, the dose can be increased considerably. That should be better investigated.”
About twenty years ago, he considered setting up a clinical trial with vitamin C himself, but he quickly abandoned that plan:
“You need a lot of doctors for such a project and the doctors I approached were not interested. People who matter in science just don’t care. I then decided that it makes more sense to continue to focus on analyzing existing data”
Reviews and meta-analysis
In his most recent meta-analysis, Hemilä showed that vitamin C increases left ventricular ejection fraction in cardiac patients. [9] He is also the lead author of a number of authoritative meta-analyses on vitamin C for the Cochrane Database of Systematic Reviews: within the medical science field the conclusions of ‘Cochrane reviews’ are often taken as the most reliable evidence.
He became best known for his Cochrane review on vitamin C and the common cold. [10] The conclusion is that vitamin C can reduce the severity and duration of a cold, albeit to a modest degree: with a daily intake of at least 1 gram of vitamin C per day an infection with a respiratory virus lasts on average 8% shorter in adults and 18% shorter in children. In 2017 he told ORTHO that you can see these results as a “proof of concept” of the effectiveness of vitamin C against respiratory infections. [1] The small but significant effect proves that vitamin C has an influence on viral infections, and there are indications that the effect is greater at higher doses. Hemilä also published meta-analyses on the effects of vitamin C on pneumonia (“therapeutic supplementation with vitamin C is reasonable”) [11] and vitamin C on the length of stay in IC patients: [12] this appears to be on average 8% shorter under the influence of moderate doses of vitamin C.
Against viral and bacterial infections
Hemilä has gradually become very well established in reference to his knowledge about vitamin C, especially with regard to infectious diseases. We should take the opinion of such a person seriously during a disruptive pandemic caused by a virus. For example, the article “Vitamin C and COVID-19,” published in the journal Frontiers in Medicine in early 2021. [13] In that article, he reviewed the evidence from about a hundred animal studies that have shown that vitamin C can alleviate a wide range of viral and bacterial infections. In mice with sepsis and acute respiratory distress syndrome (ARDS), high-dose vitamin C administration decreased pro-inflammatory genes, improved epithelial barrier function and improved alveolar fluid clearance. According to Hemilä, vitamin C has a number of biological properties that are important in light of Covid-19 and a weakened immune system: the vitamin stimulates the proliferation and function of T lymphocytes and Natural Killer lymphocytes and increases the production of interferon, which are important functions of the immune system.
Low blood levels
An important indication of the usefulness of vitamin C in the treatment of Covid-19 is the fact that patients in critical condition who end up in intensive care often have greatly reduced blood levels of vitamin C. [13] And a vitamin C deficiency is often associated with pneumonia: “While 0.1 grams of vitamin C per day can maintain a normal plasma level in a healthy person, much higher doses (1-4 grams per day) are needed for critically ill patients to raise plasma vitamin C levels to the normal range. Therefore, high vitamin C doses may be needed to compensate for the increased metabolism to reach normal plasma levels.”
Sepsis and ARDS patients
Hemilä acknowledges in the article that there are currently no large double-blind random-controlled trials that provide direct evidence for an effect of vitamin C against Covid-19. [13] Weighing his words on a gold platter, however, he states that pending more and larger studies, high-dose vitamin C administration is already known to be helpful for Covid patients. After all, the vitamin is cheap and safe. He makes a suggestion based on his own review from 2017: “In patients suffering from a viral respiratory infection, 6 to 8 grams of oral vitamin C was significantly more effective than 3 to 4 grams per day. In recent studies of sepsis and ARDS patients, the dose of intravenous vitamin C was 7 to 14 grams over 3 to 4 days.” [14]
Currently Hemilä finds that his call to utilize vitamin C has been little heeded. The fact that doctors have not started to give vitamin C to Covid-19 victims en masse can be explained by the appalling lack of good and large-scale studies. But why have they not been implemented? When asked about the state of affairs regarding the science of vitamin C and Covid-19 during the interview, he answered: “I can’t say exactly because there is so much published that I can’t keep up with it. Most of it is of low quality.”
The Chinese Vitamin C Trial (2020)
As early as mid-2020, Hemilä was asked as a reviewer to comment on the protocol of a Chinese double-blind randomized placebo-controlled study. [15] The intention of the study was that 308 Covid-19 patients in the ICU would receive 24 grams daily of vitamin C or a placebo by infusion for a week. However, the execution of the experiment largely failed because of the draconian lockdown measures of the Chinese government, and too few patients ended up in the ICU. It eventually became a ‘pilot study’ with 56 patients: the duration of artificial respiration did not decrease in the vitamin C group. [16] According to Hemilä, however, the number of test subjects was too low to draw clear conclusions. After the interview, he sent in an e-mail: “You asked about the state of affairs about vitamin C and Covid. See what you find when you type [vitamin C] and [Covid-19] on pubmed.” The scientific search engine turns out to cough up sixteen reviews and four clinical studies. Hemilä, disappointed wrote: “That says enough. And most of it is junk.”
How it started
How can the half-baked treatment of vitamin C be explained? Harri Hemilä explains it based on his own experiences over the years. His fascination for the vitamin started in the 1970s when he saw Linus Pauling on television. The two-time Nobel laureate has just published his book Vitamin C and the Common cold. In it, he argued, based on the studies available at the time, that the common cold can be treated with high doses of C. A few weeks later, a Swedish professor appeared on Finnish television. “A very arrogant man,” Hemilä recalls. “He had a bottle of vitamin C tablets with him and said, “This is junk without any effect.” But he had no factual arguments or study results to support his negative statements.”
Hemilä was studying biochemistry at the time and he asked himself who is right: Pauling or the skeptical professor? “I started collecting all the articles about vitamin C and infections. I didn’t understand how it was possible that the important reviews judged the vitamin so negatively, while you could conclude from the results of studies that C is actually effective.”
(Pim Christiaans is journalist, magazine maker and author of health books in the Dutch language. He writes about scientific developments in the field of healthy aging at his website www.lifeunlimited.nl . Christiaans has no financial ties with or interests in companies that manufacture or sell nutritional supplements.)
Translated from Dutch and reprinted in English with permission of the author and Orthomoleculair Magazine, April 2022. Those seeking permission to reprint or translate may contact the magazine’s publisher Gert Schuitemaker (ortho@ortho.nl)
References
1. Christiaans P (2017) Vitamine C tegen verkoudheid. Orthomoleculair Magazine. 5:184-189. https://docplayer.nl/154405845-Vitamine-c-tegen-verkoudheid-opnieuw-op-een-rij-gezet-door-finse-wetenschapper.html
2. Hemilä H, Chalker E (2022) Bias against Vitamin C in Mainstream Medicine: Examples from Trials of Vitamin C for Infections. Life 12:62. https://pubmed.ncbi.nlm.nih.gov/35054455.
3. Thomas S, Patel D, Bittel B, et al. (2021) Effect of high-dose zinc and ascorbic acid supplementation vs usual care on symptom length and reduction among ambulatory patients with SARS-CoV-2 infection: The COVID A to Z randomized clinical trial. JAMA Netw Open. 4:e210369. https://pubmed.ncbi.nlm.nih.gov/33576820
4. Karlowski TR, Chalmers TC, Frenkel LD, et al. (1975) Ascorbic acid for the common cold: A prophylactic and therapeutic trial. JAMA 231:1038-1042. https://pubmed.ncbi.nlm.nih.gov/163386
5. Hemilä H (1996) Vitamin C, the placebo effect, and the common cold: A case study of how preconceptions influence the analysis of results. J Clin Epidemiol. 49:1079-1084. https://pubmed.ncbi.nlm.nih.gov/8826986
6. Fowler AA, Truwit JD, Hite RD et al. (2019) Effect of vitamin C infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: the CITRIS-ALI randomized clinical trial. JAMA 322:1261-1270. https://pubmed.ncbi.nlm.nih.gov/31573637
7. Hemilä H, Chalker E (2020) Vitamin C may reduce the duration of mechanical ventilation in critically ill patients: a meta-regression analysis. J Intensive Care 8:15. https://pubmed.ncbi.nlm.nih.gov/32047636
8. Padayatty SJ, Sun AY, Chen Q, et al. (2010) Vitamin C: Intravenous Use by Complementary and Alternative Medicine Practitioners and Adverse Effects. PLoS ONE 5(7):e11414. https://pubmed.ncbi.nlm.nih.gov/20628650
9. Hemilä H, Chalker E, de Man AME (2022) Vitamin C May Improve Left Ventricular Ejection Fraction: A Meta-Analysis. Front Cardiovasc Med. 9:789729. https://pubmed.ncbi.nlm.nih.gov/35282368
10. Hemilä H, Chalker E (2013) Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev. 2013(1):CD000980. https://pubmed.ncbi.nlm.nih.gov/23440782
11. Hemilä H, Louhiala P. Vitamin C for preventing and treating pneumonia. Cochrane Database Syst Rev 2013; 8:CD005532. https://pubmed.ncbi.nlm.nih.gov/23925826
12. Hemilä H, Chalker E (2019) Vitamin C Can Shorten the Length of Stay in the ICU: A Meta-Analysis. Nutrients 2019; 11:708. https://pubmed.ncbi.nlm.nih.gov/30934660
13. Hemilä H, de Man AME (2021) Vitamin C and COVID-19. Front Med. 7:559811. https://pubmed.ncbi.nlm.nih.gov/33537320
14. Hemilä H (2017) Vitamin C and infections. Nutrients 9:339. https://pubmed.ncbi.nlm.nih.gov/28353648
15. Liu F, Zhu Y, Zhang J, et al. (2020) Intravenous high-dose vitamin C for the treatment of severe COVID-19: study protocol for a multicentre randomised controlled trial. BMJ Open 10:e039519. https://pubmed.ncbi.nlm.nih.gov/32641343
16. Zhang J, Rao X, Li Y, et al. (2021) Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann. Intensive Care 11:5. https://pubmed.ncbi.nlm.nih.gov/33420963
Nutritional Medicine is Orthomolecular Medicine
Orthomolecular medicine uses safe, effective nutritional therapy to fight illness. For more information: http://www.orthomolecular.org
Find a Doctor
To locate an orthomolecular physician near you: http://orthomolecular.org/resources/omns/v06n09.shtml
The peer-reviewed Orthomolecular Medicine News Service is a non-profit and non-commercial informational resource.
Editorial Review Board:
Albert G. B. Amoa, MB.Ch.B, Ph.D. (Ghana)
Seth Ayettey, M.B., Ch.B., Ph.D. (Ghana)
Ilyès Baghli, M.D. (Algeria)
Ian Brighthope, MBBS, FACNEM (Australia)
Gilbert Henri Crussol, D.M.D. (Spain)
Carolyn Dean, M.D., N.D. (USA)
Ian Dettman, Ph.D. (Australia)
Susan R. Downs, M.D., M.P.H. (USA)
Ron Ehrlich, B.D.S. (Australia)
Hugo Galindo, M.D. (Colombia)
Martin P. Gallagher, M.D., D.C. (USA)
Michael J. Gonzalez, N.M.D., D.Sc., Ph.D. (Puerto Rico)
William B. Grant, Ph.D. (USA)
Claus Hancke, MD, FACAM (Denmark)
Tonya S. Heyman, M.D. (USA)
Patrick Holford, BSc (United Kingdom)
Suzanne Humphries, M.D. (USA)
Ron Hunninghake, M.D. (USA)
Bo H. Jonsson, M.D., Ph.D. (Sweden)
Dwight Kalita, Ph.D. (USA)
Felix I. D. Konotey-Ahulu, MD, FRCP, DTMH (Ghana)
Jeffrey J. Kotulski, D.O. (USA)
Peter H. Lauda, M.D. (Austria)
Alan Lien, Ph.D. (Taiwan)
Homer Lim, M.D. (Philippines)
Stuart Lindsey, Pharm.D. (USA)
Pedro Gonzalez Lombana, MD, MsC, PhD (Colombia)
Victor A. Marcial-Vega, M.D. (Puerto Rico)
Juan Manuel Martinez, M.D. (Colombia)
Mignonne Mary, M.D. (USA)
Jun Matsuyama, M.D., Ph.D. (Japan)
Joseph Mercola, D.O. (USA)
Jorge R. Miranda-Massari, Pharm.D. (Puerto Rico)
Karin Munsterhjelm-Ahumada, M.D. (Finland)
Tahar Naili, M.D. (Algeria)
W. Todd Penberthy, Ph.D. (USA)
Zhiyong Peng, M.D. (China)
Isabella Akyinbah Quakyi, Ph.D. (Ghana)
Selvam Rengasamy, MBBS, FRCOG (Malaysia)
Jeffrey A. Ruterbusch, D.O. (USA)
Gert E. Schuitemaker, Ph.D. (Netherlands)
T.E. Gabriel Stewart, M.B.B.CH. (Ireland)
Thomas L. Taxman, M.D. (USA)
Jagan Nathan Vamanan, M.D. (India)
Garry Vickar, M.D. (USA)
Ken Walker, M.D. (Canada)
Anne Zauderer, D.C. (USA)
Andrew W. Saul, Ph.D. (USA), Editor-In-Chief
Associate Editor: Robert G. Smith, Ph.D. (USA)
Editor, Japanese Edition: Atsuo Yanagisawa, M.D., Ph.D. (Japan)
Editor, Chinese Edition: Richard Cheng, M.D., Ph.D. (USA)
Editor, French Edition: Vladimir Arianoff, M.D. (Belgium)
Editor, Norwegian Edition: Dag Viljen Poleszynski, Ph.D. (Norway)
Editor, Arabic Edition: Moustafa Kamel, R.Ph, P.G.C.M (Egypt)
Editor, Korean Edition: Hyoungjoo Shin, M.D. (South Korea)
Editor, Spanish Edition: Sonia Rita Rial, PhD (Argentina)
Contributing Editor: Thomas E. Levy, M.D., J.D. (USA)
Contributing Editor: Damien Downing, M.B.B.S., M.R.S.B. (United Kingdom)
Assistant Editor: Helen Saul Case, M.S. (USA)
Technology Editor: Michael S. Stewart, B.Sc.C.S. (USA)
Associate Technology Editor: Robert C. Kennedy, M.S. (USA)
Legal Consultant: Jason M. Saul, JD (USA)
Comments and media contact: drsaul@doctoryourself.com OMNS welcomes but is unable to respond to individual reader emails. Reader comments become the property of OMNS and may or may not be used for publication.
How to Tell the Difference Between Herpes and Shingles
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2024/04/23/difference-between-herpes-and-shingles.aspx
Analysis by Dr. Joseph Mercola April 23, 2024

STORY AT-A-GLANCE
- Herpes and shingles are common infections caused by herpesviruses that trigger a unique primary infection and can be reactivated later. Up to 80% of Americans have oral herpes, 1 of 6 have genital herpes and 1 in 3 will develop a shingles outbreak in their lifetime
- Shingles is a reactivation of the varicella-zoster virus that causes chickenpox. Chickenpox is highly contagious, spreading through close contact even before the rash breaks out. People with shingles can also spread the virus to people who haven’t had chickenpox
- Shingles triggers a blistered rash that crusts over and resolves within two to three weeks. The rash occurs in a stripe on one side of the body or face and typically doesn’t spread. Your risk of activation rises with age, a weakened immune system or drugs that suppress the immune system
- Oral and genital herpes spreads through close contact with fluid in the herpes blister that crusts and heals within six days. While not common, it can spread anywhere on the face or body and is triggered by events that create stress, such as a fever, physical injury, infection or surgery
- There is no cure for herpes or shingles. The best treatment is to prevent reactivation. When an outbreak occurs, keep the area clean and dry and consider supplementing with L-lysine and calcium, or licorice root
Did you know that herpes and shingles are common infections and are caused by one of the more than 100 known herpesviruses?1 While they have similarities, they are different conditions with different presentations, treatments and length of the outbreak. Identifying the correct infection may help you get quicker relief.
Eight herpesviruses routinely infect humans. These include herpes simplex virus types 1 and 2, Epstein-Barr virus, varicella-zoster virus (chickenpox), cytomegalovirus, Kaposi’s sarcoma virus and human herpesvirus 6 (types A and B) and 7.
Each herpesvirus produces a unique infection, and also has a latent period. This means the virus lives within the body without causing symptoms but can be reactivated at a later time. This latent period is characteristic of the herpesvirus.
According to Johns Hopkins Medicine,2 50% to 80% of American adults have herpes simplex virus-1 (HSV-1), commonly called just “herpes.” Typically, this causes cold sores or fever blisters in the mouth or on the lips. Herpes simplex virus-2 (HSV-2) typically causes genital herpes.
However, oral sex can spread HSV-1 into the genital area or HSV-2 to the mouth. One in 6 people in the U.S. between the ages of 14 and 49 have genital herpes, which refers to the area where the herpes outbreak occurs and not necessarily an infection with HSV-1 or HSV-2.
According to the U.S. Centers for Disease Control and Prevention,3 roughly 1 in 3 people in the U.S. will develop a shingles outbreak in their lifetime. The original infection is caused by varicella-zoster virus, also known as herpes zoster, which causes chickenpox. If you’ve ever had chickenpox, you can develop shingles, the risk for which increases as you get older, or your immune system is compromised.
How Do Chickenpox, Shingles and Herpes Spread?
Chickenpox is a highly contagious illness that spreads through close contact with someone who has chickenpox, including through coughing and sneezing4 or contact with fluid from the blisters before they are crusted and scabbed.
According to the CDC,5 without immunity, 90% of the people who get close to a person with an infection will become infected. A person is contagious one to two days before the rash appears and will remain contagious until all the lesions have crusted or scabbed. People who have been vaccinated can still develop chickenpox lesions that do not crust, and these people are also contagious.
A person with shingles can also spread the varicella-zoster virus to people who have never had chickenpox through direct contact with the fluid from the rash blisters or breathing particles that come from the blisters.6 With the first infection, these people will develop chickenpox and could then develop shingles later in life. However, people with chickenpox are more contagious than people with shingles.
Oral herpes spreads when a person has an active outbreak or sores, through intimate or personal contact.7 Since oral herpes is spread through direct contact, the best way to avoid infection is to avoid physical contact when a person is having an outbreak.
However genital herpes can spread whether there is a blister or open sore, or if there are no symptoms.8 Johns Hopkins Medicine recommends that condoms are used 100% of the time to help prevent the transmission of herpes that may happen up to 3% of the time asymptomatically. This should be weighed against monogamous couples or those who are trying to get pregnant.
Herpes and Shingles: Symptoms of Viral Activation
Since herpesviruses have a latent period, both herpes and shingles viruses stay in the body and can be reactivated after the initial infection. While the symptoms of shingles and herpes are similar, there are distinct differences. In the early hours and days of shingles reactivation, you can experience tingling in the area where the rash will eventually develop, as well as pain and itching.9
Some people notice a fever before the rash breaks out. Some of the most common characteristics of shingles is that the rash occurs in a stripe along the side of the body, localized to a particular nerve distribution and doesn’t typically spread to the rest of your body.10
It can also happen on one side of the face, affect the eye and cause vision loss. Symptoms can also include a headache, upset stomach and chills. The rash has painful fluid-filled blisters and causes the skin in the area to become reddened. The blisters begin to crust over within 10 days and all symptoms are gone within three weeks. Only 1% to 6% of people who had shingles will go on to develop a second episode.
These symptoms are quite similar to those of a herpes outbreak. The initial infection of oral herpes, also called the primary infection, is often the worst.11 It can cause flu-like symptoms, headache and swollen lymph nodes. Yet, some people may not have any symptoms with the initial infection. Later outbreaks are typically milder, and sores appear on the edges of the lips or just inside the mouth.
Symptoms include initial redness and swelling in the area where the blisters erupt. The blisters are typically painful, fluid-filled and highly infectious. After four to six days, they begin to crust over and heal. The symptoms of genital herpes are virtually identical.12 People typically describe symptoms before the lesions appear, such as a burning, tingling, itching or discomfort in the area. The blisters are painful and typically resolve on their own.
These are the two most well-known forms of herpes infections. However, HSV-1 can also trigger an outbreak anywhere on the face or body, called herpes gladiatorum (Mat Herpes).13 When HSV-1 infects the eye, it requires immediate medical attention. As with other HSV-1 infections, it is spread through direct skin contact with the lesion or sharing objects such as cups, eating utensils, cell phones or lip balm.
Save This Article for Later – Get the PDF Now
What Causes Herpes and Shingles to Activate?
There are specific factors that place you at greater risk for reactivating varicella-zoster (shingles), HSV-1 or HSV-2. Roughly 50% of people who live to age 85 will experience one episode of shingles.14 Your risk of shingles may increase in these circumstances:15
- Over the age of 50
- Weakened immune system from illness or trauma
- Autoimmune disease
- Drugs that suppress your immune system
Other factors that can disturb your immune system have also been found to trigger a shingles outbreak. As I reported in January 2023, several case studies and one systematic review of the literature found that the COVID jab increased the risk of shingles reactivation if you had it before or had a known risk factor for it.
The shots suppress your innate immune system, which is the first stage of response for all viral infections. When this pathway is suppressed, latent viruses can begin to emerge. A shingles outbreak can lead to complications, the most common of which is postherpetic neuralgia, or long-term nerve pain.
Pain occurs over the area of the skin where the rash was located and can last for months or years. According to the CDC,16 up to 18% of people who have shingles will develop postherpetic neuralgia, and older adults are more at risk of having-longer lasting and more severe pain.
Shingles can also lead to other serious complications when the rash involves the eye, including loss of your eyesight. People with a weakened immune system have a higher risk of complications, including a secondary bacterial infection, hearing problems, lung infection, brain inflammation and death.
The specific factors that trigger herpes reactivation are not clear, but recurrent outbreaks tend to become fewer after the first year as your body develops antibodies to the virus. Situations that may trigger an occurrence of either oral or genital herpes include:17,18
| Fever | Stress | Menstruation | Physical injury |
| Infection | Sunburn | Surgery |
Is There Treatment for Herpes or Shingles?
At this time, there is no known cure for any of the herpes viruses, including HSV-1, HSV-2 or varicella-zoster virus. The best treatment is to take consistent steps to prevent reactivation. Both viruses have a higher rate of reactivation when your body is under stress, or your immune system is compromised. Consider the simple steps you can take every day to help you take control of your health.
For example, when possible, choose a whole-food diet and eliminate or significantly reduce processed foods. These are known to be high in linoleic acid, which is highly destructive to your health. Take steps to reduce your stress levels by practicing yoga, meditation, journaling or another activity of your choice. Include exercise in your daily habits, which can also help to reduce stress and support your overall health.
Johns Hopkins Medicine19,20 lists specific treatments that your healthcare provider might recommend for oral and genital herpes, including antiviral oral medications or topical ointments. It’s also important to keep any area clean and dry to reduce the risk of a secondary infection.
For those with genital herpes, using a sitz bath or sitting in a warm bathtub for approximately 20 minutes can help reduce the discomfort. Take care to avoid any scented or soap products in the bathtub. Wet compresses, warm oatmeal baths and calamine lotion can also help relieve the itching and soothe your skin with shingles.
Other options include treatments that have been shown to interrupt the replication of viruses, including lysine supplementation and licorice root. Lysine is an essential amino acid used in the production of protein, which virologists suggested could help prevent or treat viral illnesses in 2020,21 since it had demonstrated this property in the past.
In studies evaluating the effectiveness of L-lysine against herpes, it demonstrated an ability to reduce the average number of infections and diminish the severity and healing time.22 A 2017 study23 noted that dosages needed to be 1 gram per day or more with a diet low in arginine to effectively help prevent an outbreak, since HSV uses arginine to reproduce.
It would also be wise to take a little extra calcium with the L-lysine. Calcium plays several critical roles in the body’s response to viral infections. For example, calcium ions act as key signaling molecules within cells. During a viral infection, signaling pathways involving calcium are crucial for activating immune cells, including T cells and macrophages. These cells are essential for identifying and eliminating viral pathogens from the body.
Another option is licorice root, which has been a formidable antiviral agent in the fight against herpes, hepatitis and influenza.24 Glycyrrhizin is the bioactive ingredient that has demonstrated antiviral properties.
Herpes and Shingles: Side-by-Side Comparison
As you’ve noticed, while there are similarities, there are also significant differences. By correctly identifying the viral infection, you can estimate the length of the outbreak, watch for complications and seek the correct care. Here’s a quick side-by-side comparison that includes the information we just discussed.
| Factor | Herpes | Shingles |
|---|---|---|
| Virus | Herpes simplex virus-1 (HSV-1) and HSV-2 | Varicella-zoster virus |
| Transmission | Close contact with fluid from the blisters | Close contact before the rash appears (cough and sneeze) and with fluid from the blisters after eruption |
| Symptoms | A small cluster of lesions that are painful, blister and crust over in roughly four to six days.
They commonly appear in or around the mouth or genitals but can appear anywhere on the face or body |
Red, painful rash that blisters before crusting over in 10 days and resolves in three weeks.
The rash occurs in stripes on one side of the body or face. Other symptoms can include a fever, headache and chills |
| Triggers | Trauma to the area, physical injury, surgery, fever, stress, infection, sunburn, menstruation | Weakened immune system from medications or illness; incidence increases with age |
| Complications | Loss of eyesight if it affects the eye | Post-herpetic neuralgia (nerve pain), eyesight loss if shingles affect the eye, secondary bacterial infection, hearing problems, lung infection and brain inflammation |
| Treatment | No known cure; people with genital herpes may experience relief with 20-minute warm soaks.
Antiviral medications can be prescribed. May also get relief with a diet low in arginine in addition to L-lysine supplementation |
No known cure; physicians typically prescribe antiviral medications.
L-lysine and low arginine diet demonstrate effectiveness in other herpes infections including oral and genital herpes |
– Sources and References
- 1 Medical Microbiology, Chapter 68: Herpesviruses, para 1
- 2 Johns Hopkins Medicine, Herpes: HSV-1 and HSV-2
- 3 Centers for Disease Control and Prevention, Shingles (Herpes Zoster) first purple block
- 4 New York State Department of Health, Chickenpox, subhead 3
- 5 Centers for Disease Control and Prevention, Chickenpox, Transmission
- 6, 15 Centers for Disease Control and Prevention, Shingles, Cause and Transmission
- 7 Johns Hopkins Health, Oral Herpes, Subhead 1
- 8 Johns Hopkins Health, Genital Herpes – How Does Genital Herpes Spread? 50% DTP and Do condoms prevent the spread
- 9 Centers for Disease Control and Prevention, Shingles, Signs and Symptoms
- 10 Nebraska Medicine, What do shingles look like and where do they come from? Subhead 2
- 11 Johns Hopkins Health, Oral Herpes, Subhead 3
- 12, 17 Johns Hopkins Health, Genital Herpes, Subhead 6
- 13 New York Department of Health, Viral Skin Infections: Herpes Gladiatorum
- 14 Nebraska Medicine, What do shingles look like and where do they come from? Subhead 5
- 16 Centers of Disease Control and Prevention, Shingles, Complications
- 18 Johns Hopkins Health, Oral Herpes, Subhead 5
- 19 Johns Hopkins Health, Oral Herpes, Last subhead
- 20 Johns Hopkins Health, Genital Herpes – Can genital herpes be treated? 65% DTP
- 21 Research Gate, September 2020
- 22 Dermatologica, 1987;175(4):183-90
- 23 Integrative Medicine: A Clinician’s Journal, 2017; 16(3) Abstract – Results/Conclusion and 1st para after Conclusion
- 24 Acta Pharmacology, 2015;5(4) 2.1 GL para 7, 45% DTP
HIV mRNA Vaccines Continue to Fail in Clinical Trials
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2024/04/24/hiv-mrna-vaccine-clinical-trials.aspx
Analysis by Dr. Joseph Mercola April 24, 2024

STORY AT-A-GLANCE
- The most recent mRNA failure was a phase 1 trial of Moderna’s mRNA human immunodeficiency virus (HIV) injection
- Larger trials were halted after a high rate of “puzzling skin side effects” occurred
- In a series of phase 1 trials, 7% to 18% of participants who received the experimental mRNA shots experienced skin reactions, including hives, itchiness or hives caused by scratching
- Skin reactions can be an “early warning radar for general immune response” indicative of a greater problem
- Although all HIV mRNA shots have failed to pass even the initial trials, we’re to believe COVID-19 mRNA shots passed safety and efficacy studies with flying colors and the technology is thereby “proven” safe and effective
Messenger ribonucleic acid (mRNA) vaccines are being described as a “new era in vaccinology.”1 Research is underway to develop mRNA shots for not only coronaviruses but also C. difficile, hepatitis C, influenza, malaria, norovirus, cancer and more2 — despite the fact that all mRNA shots are likely ineffective and/or dangerous.
The most recent mRNA failure was a phase 1 trial of Moderna’s mRNA human immunodeficiency virus (HIV) injection. Larger trials were halted after a high rate of “puzzling skin side effects” occurred.
“We are taking this very seriously,” Carl Dieffenbach, head of the Division of AIDS at the National Institute of Allergy and Infectious Diseases (NIAID), told Science.3 Although all HIV mRNA shots have failed to pass even the initial trials, researchers plan to repeat the phase 1 trial using a lower dose.
High Rates of Skin Reactions Halt HIV mRNA Shot Trials
Trials of mRNA-based HIV immunogens are being conducted in partnership by the International AIDS Vaccine Initiative (IAVI), Moderna, the HIV Vaccine Trials Network (HVTN), the National Institutes of Health (NIH) and the Bill & Melinda Gates Foundation.4
In a series of phase 1 trials, 7% to 18% of participants5 who received the experimental shots experienced skin reactions, including hives, itchiness or hives caused by scratching. In a news release, IAVI largely downplayed the concerning outcome, stating:6
“Most of these events were mild or moderate, and managed with simple allergy medications. There were no serious adverse events reported. Participants who experienced skin events were provided all medical care necessary and were monitored closely.
IAVI and partners are actively working to investigate the potential causes of these skin events. We have brought in an interdisciplinary team of external experts, including allergists and immunologists, to further assess the skin events.
In the interest of transparency and clarity, IAVI and partners have presented preliminary data on immune responses and safety at scientific conferences and look forward to continuing our discussion of these results.”
However, the setback highlights the continued failures in the race to create an mRNA HIV shot. “We would be moving more quickly if this finding had not been observed,” IAVI head Mark Feinberg told Science.7
Problems Plague mRNA HIV Shots
To create the shot, researchers have been injecting “different mRNAs, encoding various pieces of HIV’s surface protein or the entire molecule, over the course of several months.”8 The idea is to trigger the creation of broadly neutralizing antibodies, or bNAbs.
BNAbs are immune system proteins that have the unique ability to fight a wide range of strains of a virus. In terms of HIV, bNAbs are of particular interest because HIV is highly variable, with numerous strains circulating globally. Derek Lowe, a medicinal chemist, wrote:9
“Moderna has been working for some years now on a possible HIV vaccine using their mRNA technology, which is an ambitious goal. There have been numerous attempts at this over the decades, and needless to say none of them have worked out yet. There is almost certainly not going to be a single-shot vaccine targeting a single antigen — the situation is too complex for that.
Since the virus comes in many different strains, the hope has been that some sort of more comprehensive vaccine protocol might be able to induce broadly neutralizing antibodies that could take on all comers.”
Most antibodies target specific virus strains, but bNAbs can neutralize many strains of HIV, making them a powerful tool in the fight against this virus. While people with HIV sometimes develop their own bNAbs, no vaccine has done so.10
The idea in creating bNAbs through mRNA technology for HIV is to deliver instructions for creating proteins that resemble parts of the HIV envelope. This would, in theory, stimulate the immune system to produce bNAbs that can neutralize a wide range of HIV strains, offering a broad protection against the virus. As reported by Bloomberg:11
“Creating an mRNA vaccine for HIV is trickier than making the kind of SARS-CoV-2 shots we’ve become familiar with. The mRNA COVID vaccines deliver the recipe for the spike protein … This causes immune cells to produce neutralizing antibodies against COVID, much as they would do if they had experienced a COVID infection.
With HIV, there’s no such simple recipe. HIV’s equivalent to the spike protein — its envelope glycoprotein — is wilier. It hides its vulnerable aspects, making it difficult for immune cells to generate antibodies against it. An even bigger problem is that HIV starts to mutate within hours of infecting someone …
HIV behaves like ‘a swarm of slightly different viruses’ … People with HIV rarely develop neutralizing antibodies, and in the very few who do, the antibodies take years to evolve — far too long for them to effectively fight the virus. The immune system can’t keep up.
But what if the immune system could be given a head start? That’s the idea behind the Moderna/IAVI vaccine … The researchers will administer a series of shots to try to coax the immune system along that years-long process ahead of time so that when it is exposed to HIV, it can spring into action.”
Save This Article for Later – Get the PDF Now
Skin Problems May Be Early Warning for an Immune Response
While the Moderna HIV shot reportedly generated “impressive antibodies that were moving toward bNAbs,”12 the high rate of skin problems it triggered are suggestive of a greater problem. Lowe went so far as to describe them as an “early warning radar for general immune response”:13
“A significant number of vaccine recipients (ten to fifteen percent in some cases) have shown various sorts of skin reactions (hives, etc.) These almost always resolve, but it is a warning.
Skin reactions are sort of an early warning radar for general immune response (thus the skin tests for various allergens), and the worry is that these might well become worse on further dosing (or be harbingers of other immune problems in different organ systems). It’s definitely worth a closer look.
I have to point out that this side effect rate is much higher than has been seen with the coronavirus mRNA vaccines (thus the alarm bells), but skin reactions are not unknown there, either … No one is quite sure if it’s the mRNA species themselves that set off the response here, or if it’s something about the formulation (the lipid nanoparticles).”
“Potentially more worrisome, however, would be if the problem is tied to a cumulative effect from multiple mRNA shots,” Science reported.14 It’s important to point out that while all HIV mRNA shots have failed, we’re to believe COVID-19 mRNA shots passed safety and efficacy studies with flying colors and the technology is thereby “proven” safe and effective.
But as noted by Canadian oncologist and cancer researcher Dr. William Makis, “The more mRNA shots you take, the greater the immune system damage, the greater your risk of impaired cancer surveillance and hence, the greater your risk of turbo cancer.”15
Turbo cancers is a term used to describe the emergence of rapid-growing cancers in people, many under age 30, who have received one or more COVID jabs — another warning that mRNA shots aren’t as safe as we’ve been led to believe. Makis tweeted:16
“Unfortunately, the entire LNP/mRNA Vaccine field is a fraud. It’s a failed technology with an unacceptably terrible side effect profile. The entire field now depends on the suppression of COVID-19 mRNA Vaccine injuries & deaths, which are now in the millions (5.3 million in WHO VigiAccess alone), so we are no longer dealing with scientists but con artists …
They are trying to find “novel” ways to market a failed technology platform and sneak failed vaccine products onto the market. The Moderna HIV mRNA Vaccine is such a product … And yes, they are moving forward, despite 20% of HIV mRNA Vaccine Victims developing skin rashes in Phase I trials. Moderna will repeat the Phase I trials with a slightly lower dose. The poisonings will continue until vaccine injuries improve.”
All mRNA Shots Likely Ineffective, Dangerous
While the latest HIV mRNA shot trial showed a risk of side effects, others have shown the shots don’t work. One clinical trial conducted by the NIAID-funded HIV Vaccine Clinical Trials Network began in 2019 and involved 3,900 participants. The experimental HIV vaccine regimen used in the study was developed by Janssen, the vaccine division of Johnson & Johnson, and did not provide protection against HIV, leading the study to be discontinued.17
“The vaccine used the same antigen delivery system employed by J&J’s COVID-19 vaccine, a common cold virus known as adenovirus 26,” Stat News reported, and at least five others have also failed. While the Janssen HIV shot was not mRNA, the HIV Vaccine Trials Network continued to point to mRNA technology as a potential solution.18 However, mRNA shots are inherently problematic.
For instance, Pfizer’s mRNA COVID-19 shots also instruct cells to produce additional “off-target” proteins that could pose significant health risks. Ribosomes decode mRNA in cells, but about 8% of the time those in COVID-19 shots may misread the coded instructions, Maryanne Demasi, Ph.D., a former medical scientist with the University of Adelaide and former reporter for ABC News in Australia, explains:19
“The researchers say that ribosomes, which are responsible for decoding the mRNA in cells, can slip and misread the coded instructions about 8% of the time – known as ‘ribosomal frameshifting.’ They say the ‘glitch’ has to do with how the mRNA in the vaccine has been genetically modified.
Unlike naturally-occurring mRNA, the mRNA that exists in the vaccines has had a ‘uridine’ base replaced with a ‘N1-methyl pseudouridine’ (to stabilise it) and unfortunately, has made it prone to reading errors.”
In May 2021, I interviewed Stephanie Seneff, Ph.D., a senior research scientist at MIT for over five decades, about the likely hazards of replacing the uracil in the RNA used in the COVID shots with synthetic methylpseudouridine.20 This process of substituting letters in the genetic code is known as codon optimization, which is known to be problematic.
At the time, Seneff predicted the shots would cause a rise in prion diseases, autoimmune diseases, neurodegenerative diseases at younger ages, blood disorders and heart failure, and one of the primary reasons for this is because they genetically manipulated the RNA in the shots with synthetic methylpseudouridine, which enhances RNA stability by inhibiting its breakdown.
Researchers at Cambridge University and the Universities of Kent, Oxford and Liverpool, then discovered21 that the use of methylpseudouridine results in a high rate of ribosomal “frameshifting,” which causes your cells to produce off-target proteins with unknown effects.
Further, in a 2023 preprint study, microbiologist Kevin McKernan — a former researcher and team leader for the MIT Human Genome project22 — and colleagues assessed the nucleic acid composition of four expired vials of the Moderna and Pfizer mRNA shots.
“DNA contamination that exceeds the European Medicines Agency (EMA) 330ng/mg requirement and the FDAs 10ng/dose requirements” was found.23 So, in addition to the spike protein and mRNA in COVID-19 shots, McKernan’s team discovered SV40 promoters that, for decades, have been suspected of causing cancer in humans.24
Injured by an mRNA COVID Jab? Here’s Help
It’s important to be wary of any new mRNA shots that come on the market and carefully weigh if the risks outweigh the reported benefits before getting on. However, if you’ve already had one or more COVID-19 shots, there are steps you can take to repair from the assault on your system.
Remember, the more mRNA shots you take, the greater the immune system damage. So, the first step is to avoid getting anymore mRNA jabs. Next, if you’ve developed any unusual symptoms, seek out help from an expert. The Front Line COVID-19 Critical Care Alliance (FLCCC) also has a treatment protocol for post-jab injuries. It’s called I-RECOVER and can be downloaded from covid19criticalcare.com.25
Dr. Pierre Kory, who cofounded the FLCCC, has transitioned to treating the vaccine injured more or less exclusively. For more information, visit DrPierreKory.com. Board-certified internist and cardiologist Dr. Peter McCullough is also investigating post-jab treatments, which you can find on PeterMcCulloughMD.com.
- 1 Nature Reviews Drug Discovery January 12, 2018
- 2 Penn Medicine, mRNA Vaccines
- 3, 7, 8, 10, 12, 14 Science March 1, 2024
- 4, 5, 6 IAVI March 2, 2024
- 9, 13 Science March 11, 2024
- 11 Bloomberg February 4, 2022 (Archived)
- 15 Rumble, The HighWire with Del Bigtree, Is the COVID Vaccine Causing Turbo Cancers? September 22, 2023
- 16 X, William Makis MD March 18, 2024
- 17 NIH January 18, 2023
- 18 Stat News January 18, 2023
- 19 Maryanne Demasi Reports January 16, 2024
- 20 International Journal of Vaccine Theory, Practice and Research May 10, 2021; 2(1): 402-444
- 21 Nature volume 625, pages 189–194 (2024)
- 22 The Healthcare Channel May 22, 2023
- 23 OSF Preprints April 10, 2023
- 24 Expert Rev Respir Med October 2011; 5(5): 683-697
- 25 Covid19criticalcare.com