Shingles
now browsing by category
DMSO Transforms the Treatment of Infectious Diseases
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2025/01/17/dmso-infectious-diseases.aspx
Analysis by A Midwestern Doctor January 17, 2025

STORY AT-A-GLANCE
- Dimethyl sulfoxide (DMSO) is a safe, naturally occurring substance with properties that make it effective for treating various medical conditions, including pain, injuries, wounds, strokes, spine injuries, autoimmune disorders, cancer, and internal organ diseases
- DMSO has broad antimicrobial properties, protects against microbial toxins, combats antibiotic resistance, and helps deliver healing deep into the body to treat otherwise inaccessible infections
- DMSO studies have generated evidence supporting its role in treating cancer and autoimmune disorders through its unique antimicrobial properties
- DMSO is highly effective against viruses like herpes and shingles, as well as conditions like feline panleukopenia in cats
- DMSO also proves valuable in treating persistent fungal and parasitic infections
Introduction
DMSO is a remarkably safe and naturally occurring substance (provided you use it correctly1) that rapidly improves a variety of conditions medicine struggles with — particularly chronic pain. For reference, those conditions included:
| Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here. |
| A wide range of tissue injuries such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here). |
| Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here. |
| A wide range of autoimmune, protein, and contractile disorders such as scleroderma, amyloidosis, and interstitial cystitis (discussed here). |
| A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here). |
| A wide range of internal organ diseases such as pancreatitis, infertility, liver cirrhosis, and endometriosis (discussed here). |
| A wide range of skin conditions such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here). |
In turn, since I started this series, it struck a cord and I have received over 1400 reports of remarkable responses to DMSO many readers have had (compiled here).
This begs an obvious question — if a substance capable of doing all of that exists, why does almost no one know about it? Simply put, like many other promising therapies, it fell victim to a pernicious campaign by the FDA which kept it away from America despite decades of scientific research, Congressional protest, and thousands of people pleading for the FDA to reconsider its actions. Consider for example, this 60 Minutes program about DMSO that aired on March 23, 1980:
DMSO and Infectious Diseases
DMSO has a variety of unique therapeutic properties. Some of those make it incredibly well-suited to addressing microbial infections. For example:
• While nontoxic, it has an antiseptic effect that is harmful to microorganisms, especially the smallest ones. This property appears to be the most beneficial for herpes, shingles, and complex conditions with a microbiological component.
• It can remove the antibiotic resistance of bacteria. This is particularly helpful in widespread problematic infections that have gradually developed a resistance to many existing antibiotics (e.g., tuberculosis) and challenging infections that are not responding to antibiotics (e.g., ones that would otherwise require an amputation).
• It can deliver antimicrobial agents to areas that are typically difficult to reach (e.g., deep in a bone) and also directly to regions that would otherwise require a systemic application of the medication.
• It can increase circulation to many parts of the body, something which is often critical for resolving illnesses (as a healthy blood supply allows the immune system to enter and heal diseased areas). Likewise, pretreatment with DMSO has been shown to increase the immune system’s ability to resist a subsequent infection.
• Much in the same way DMSO protects cells from a wide variety of lethal stressors,2 it can also protect them from the harmful effects of bacterial toxins and can mitigate the toxicity of antimicrobial agents taken for a prolonged period.
In short, DMSO can transform the management of infectious diseases.

Save This Article for Later – Get the PDF Now
Shingles and Herpes
Since many people struggle with Herpes (HSV-1 or HSV-2) and Shingles (Herpes Zoster), especially the pain which follows shingles (known as post-herpetic neuralgia or PHN), DMSO has been extensively studied for these uses. In turn, DMSO was found to significantly improve those conditions (and canker sores3), particularly when combined with idoxuridine (IDU), an antiviral that has poor penetration into tissues (and hence does not work alone).
• Herpes simplex
◦A 1965 study4 used 1% IDU in 90% DMSO (and 10% distilled water) in 7 patients with severe cutaneous infections and noted significant improvement in all herpes cases, with the only side effect being slight skin irritation from the solution.
◦A 1966 RCT5 (randomized controlled trial) of 21 patients with recurrent herpes found DMSO halved the durations of outbreaks, and when given with 5% idoxuridine, cut it to a third (with similar results also found in a 1967 study6).
◦A 1983 study7 found that DMSO effectively brought acyclovir (ACV) into the skin, caused a moderate reduction in herpes lesions, and dramatically reduced them when combined with acyclovir.
◦A 1990 RCT8 gave 80% DMSO mixed with 15% IDU to 301 immunocompetent female patients. The duration of pain was reduced by 2.6 days and the healing time to normal skin by 2.3 days.
◦A 2002 cell study9 found 0.65% DMSO reduced herpes viral replication by 50%.
Note: DMSO also helps herpes fever blisters, and DMSO with IDU has been reported to be effective in treating HSV whitlow (herpes on the fingers).10

• Shingles and Post Herpetic Neuralgia (PHN)
◦In 1967, a German investigator reported DMSO yielded generally good results in 10 of 11 shingles and PHN cases11 (with similar results being found in another 1967 study12).
◦Two 1970 RCTs showed that IDU in DMSO was at reducing the duration of pain and healing in shingles.13 The patients were delighted, for the pain disappeared within a median of two days.
◦In 1971, Dr. William Campbell Douglass conducted a study of 41 patients with shingles and PHN of whom 73.3% had a good response to DMSO and 13.3% had a fair response.
◦A 1974 RCT14 of 118 shingles patients and a 1992 RCT15 of 171 shingles patients found DMSO and IDU significantly shortened the vesicular phase, healing time, and duration of pain, and it significantly improved post-herpetic neuralgia.
◦A 1981 trial of 46 shingles patients also confirmed the benefit of DMSO and IDU.16
DMSO and Bacterial Infections
DMSO has five key properties that make it effective in treating bacterial infections:
1. Increased bacterial membrane permeability — DMSO enhances bacterial membrane permeability,17 making bacteria more vulnerable to antibiotics, especially those targeting internal structures (e.g., penicillin). This is crucial for treating infections like tuberculosis, which has a tough outer barrier.
2. Direct bacterial breakdown — DMSO can dissolve bacteria, causing their contents to leak out and effectively neutralizing them.
3. Disruption of bacterial function — DMSO interferes with bacterial metabolism by blocking the production of essential membrane proteins, as shown in studies with E. coli.18
4. Improved circulation — DMSO enhances blood flow,19 which helps combat chronic infections often caused by impaired circulation.
5. Protection against bacterial toxins — DMSO mitigates the harmful effects of bacterial toxins, protecting cells from stress.
DMSO also enhances the immune response,20 contrary to concerns about immune suppression, and has been shown to increase resistance to infections like typhus.21
Common Microbes
DMSO has been extensively tested against common infectious bacteria (e.g., staph, strep, E. coli, pseudomonas), both by itself and in combination with antimicrobial therapies.
After a 196422 study showed DMSO inhibited the growth of bacteria, a 1967 study tested it against various microorganisms, and found at sufficient concentrations that DMSO caused those organisms to dissolve into a sediment.23

A 1969 study24 found that 75% DMSO was bactericidal (mainly by causing their internal contents to leak out), while 15% was sufficient to stop bacterial growth.

DMSO and Head Infections
Since DMSO is effective in eliminating many common microbial infections, it has shown great promise in ENT (ears, nose, and throat) medicine, as many of those diseases result from infections with common bacteria and the inflammatory response to them (particularly since it is often challenging to get antibiotics to the site of the infection).
Much of this was demonstrated in the 1967 publication25 by an ENT doctor who observed that DMSO would often significantly calm inflammation from an infection in the head (including severe ones that were difficult to treat with antibiotics). He compiled all of his cases26 here:

• Eye infections — DMSO can treat various eye conditions, including macular degeneration and eyelid inflammation. In a 1976 study,27 it was combined with antibiotics to successfully treat eye infections. Additionally, DMSO can resolve pink eye after just a few applications.28
• Sinusitis — DMSO helps open blocked nostrils quickly by reducing swelling and promoting tissue healing.29 Studies have shown DMSO significantly alleviates sinusitis symptoms, including one 1967 study30 where most patients had excellent results. It also enhances the effectiveness of antibiotics in treating rhinoscleroma,31 a rare nasal infection.
• Dentistry — DMSO is used in dentistry as a mouthwash, relieving gum pain32 and preventing bleeding. It can alleviate toothache pain and reduce swelling after dental procedures.33 Dentists have found it effective for treating infections and saving loose teeth from periodontitis.34 Many studies35 show DMSO helps improve gum health, treat pulpitis,36 and accelerate healing after tooth extractions.37
Tuberculosis
Despite over a century of work, Tuberculosis remains the world’s most deadly microbe (e.g., in 2023, it was estimated38 to have killed 1.25 million people). This is mainly due to this tiny bacteria’s unique characteristics and high aptitude for developing antibiotic resistance.
Because of this, once the early DMSO researchers realized that DMSO could remove antibiotic resistance, their focus immediately went to tuberculosis. In turn, many lab studies39 have demonstrated DMSO’s utility for this challenging infection which has been corroborated in humans:
• A 1969 study40 of 32, 14 showed an absence of tuberculosis secretion and most showed improvement (e.g., reduced endobronchitis, perifocal infiltration and lung tissue destruction).
• A 1980 study41 used DMSO to treat children with pulmonary tuberculosis.
• A 1991 study42 found nebulized DMSO mixed with rifampin over 1 to 2 months was an effective treatment for 148 pulmonary tuberculosis and 18 obstructive bronchitis patients (e.g., it healed the destructive cavities caused by tuberculosis).
Bacterial Toxins
One of the primary reasons bacterial infections sicken and kill is because of the toxins they release. DMSO in turn, has been repeatedly shown to mitigate this. For example:
• DMSO has been shown43 to protect the duodenum from H. pylori induced chronic ulcers.
• In rats, DMSO was shown44 to create a dose dependent reduction in the fluid secretion and mucosal permeability triggered by C. difficile’s toxin (with its maximum inhibition occurring at a 1% concentration). Given how common C. difficile colitis is, this application of DMSO has great promise.
• DMSO was shown to protect cells45 from the shigella bacteria’s toxin46 (which causes severe diarrhea and bloody stools).
• Endotoxaemia occurs in response to bacterial lipopolysaccharide (LPS) entering the bloodstream. A 2008 study of 18 horses47 found DMSO reduced the fevers that followed artificially induced endotoxemia, suggesting DMSO’s utility in treating sepsis, particularly since, DMSO can protect cells48 from the damage LPS causes.
Note: One of the most important characteristics the early adopters of ultraviolet blood irradiation recognized about it was that UVBI could effectively neutralize toxins in the bloodstream (a property that saved a significant number of lives).
Challenging Infections
DMSO has shown promise for many other challenging infections:
| Sepsis — DMSO has proven effective in treating septic complications, especially in heart attack survivors. A 1982 study49 showed its success even against antibiotic-resistant bacteria. In 1984 a Russian study50 confirmed DMSO accelerated recovery in critically ill septic patients, with one case of bladder infection improving after using DMSO.
Note: One author cited51 a case of a septic patient with a severe bladder infection who did not respond to antibiotics but recovered once he began taking one teaspoon of DMSO three times a day. |
| Lung infections — DMSO has treated chronic lung infections, with a 1975 study52 showing rapid recovery in infants with severe respiratory diseases when combined with antibiotics. A 2020 study53 reported that DMSO, combined with ceftriaxone, helped 31 lung abscess patients fully recover without recurrence.
Note: DMSO has also been repeatedly shown54 to effectively treat acute respiratory distress syndrome, a challenging lung condition that frequently follows severe infections and often requires ventilation. |
| Abdominal infections — DMSO, combined with antibiotics, has effectively treated peritonitis55 and abdominal abscesses.56 It helps concentrate antibiotics in the abdomen,57 providing extended treatment duration, especially for peritonitis, a fatal condition. |
Meningitis
|
| Osteomyelitis — DMSO has shown significant results in treating bone infections.60 Studies have found that combining DMSO with antibiotics and other therapies like hyperbaric oxygen speeds up recovery and reduces bone damage in both acute and chronic osteomyelitis.61,62,63,64,65,66 |
| Orchitis and epididymitis — In 1986, a Russian physician reported these conditions have an excellent response to DMSO.67 |
| Cancer and autoimmunity — DMSO has been observed to eliminate the unusual bacteria associated with many cancers and autoimmune diseases, which may in part explain its utility for those conditions.
Note: A wealth of evidence also supports DMSO’s use in a variety of challenging veterinary infections.68 |
Surgery
Three of the major issues encountered in surgery are:
- Surgical wounds (or burns) become infected before they seal and heal.
- Infections deep within the body need to be cut open so the infection can be drained or removed (or have antibiotics directly applied to it).
- Infected tissues must be removed (e.g., amputated) because the infection within them can’t be reached or addressed.
Fortunately, DMSO’s is uniquely suited to address each of these. For example, in this article, I discussed how many studies and reader testimonials show DMSO is a remarkable therapy for burns and wound healing, and here I reviewed the wealth of evidence that DMSO is a highly effective therapy for surgical scar healing.
Likewise, DMSO makes reaching a deep infection within the body possible without surgery. Numerous studies, in turn, demonstrate that DMSO can prevent and treat those infections:
| A 1969 case report69 highlighted a patient with a chronic fungal infection (that has high resistance to antifungals) who declined amputation in favor of antifungals dissolved in DMSO which saved his foot.
Note: There are many other cases of DMSO curing a chronic infection that had required amputation.70 |
| A 1978 surgical study71 used DMSO in combination with antibiotics to treat inflammatory infiltrates. |
| A 1984 study72 used DMSO to treat surgical wound infections. |
| A 1985 study73 found that injecting DMSO after severe mechanical trauma reduces the risks of a subsequent infection, while a 1984 study74 found that DMSO plus antibiotics prevent open wounds in the hands from developing purulent infections. |
| A 1990 study75 of 33 patients with phlegmons (inflamed areas under the skin) throughout the body found that a dressing with DMSO and silver nitrate, when compared to those receiving standard treatments, reduced the time required to begin a surgical repair by 2 to 2.5 times. |
| In 1998, Russian physicians reported that they routinely apply DMSO to surgical wounds as it accelerates healing and provides general infection control.76 |
Fungal Infections
A 2013 study77 used DMSO and antifungal agents on six different Candida species. It found 0.5% to 1% DMSO had an antifungal effect, but the inhibitory effect (with or without concurrent antifungals) varied significantly.
DMSO can also effectively bring antifungals to many parts of the body. DMSO for instance was shown78 to significantly increase the amount of ketoconazole that enters the brain and can transport griseofulvin79 through the skin (which in a 1974 study80 was used to successfully treat ringworm). Additionally:
- A 1965 study81 found DMSO was an effective treatment for ringworm and athlete’s foot, especially when combined with an antifungal.
- A 1977 study82 found DMSO (in combination with lidase) was a highly effective treatment for actinomycosis of the face and neck.
- A 1997 study83 found DMSO mixed with itraconazole treated fungal infections in horse corneas.
Parasites
There is also some data on how DMSO can treat parasites (e.g., 3% DMSO has been shown to significantly inhibit the growth of Trypanosoma cruzi,84 which causes Chagas disease). However, its primary value is bringing an antiparasitic medication to the region of infection (as parasites can often burrow quite deep into the tissues).
For example, two different 1966 studies (this study85 and this 25 person RCT86) found that DMSO plus an antiparasitic (e.g., 2% topical thiabendazole in 90% DMSO) was an effective treatment for hookworm infections in the skin. DMSO can also be combined with antiparasitic medications to reach challenging parasitic infections deep within the body. For example, a 1984 case report87 discussed DMSO treating a complex amoeba infection of the liver.
Conclusion
Many who’ve worked with DMSO believe it should be routinely utilized for severe infections, particularly those not responding to antibiotic therapy. Fortunately, we are in a unique moment where these forgotten sides of medicine finally have a chance to see the light of day.
Thus, I sincerely hope articles like these can begin to shift the medical system towards adopting a more sophisticated approach to infectious diseases that can help patients struggling with challenging infections.
Author’s Note: This is an abridged version of a longer article that goes into greater detail on the points discussed here and provides guidance for personal DMSO use (e.g., dosing, therapeutic precautions and where to obtain it) along with other natural approaches we’ve also found help many of those conditions (e.g., herpes and shingles). That article can be read here.
A Note from Dr. Mercola About the Author
A Midwestern Doctor (AMD) is a board-certified physician from the Midwest and a longtime reader of Mercola.com. I appreciate AMD’s exceptional insight on a wide range of topics and am grateful to share it. I also respect AMD’s desire to remain anonymous since AMD is still on the front lines treating patients. To find more of AMD’s work, be sure to check out The Forgotten Side of Medicine on Substack.
- 1 The Forgotten Side of Medicine, October 12, 2024
- 2, 19 The Forgotten Side of Medicine, September 15, 2024
- 3 Amazon, The DMSO Handbook: A New Paradigm in Healthcare
- 4 Ohio State Med J. 1965 Jun:61:532-3
- 5 Brit. Med. J., 1966, 2, 805-807
- 6 Annals of the New York Academy of Sciences, 141: 428-436
- 7 Annals of the New York Academy of Sciences, 411: 28-33
- 8 J Infect Dis. 1990 Feb;161(2):191-7
- 9 BMC Infect Dis. 2002 May 24:2:9. doi: 10.1186/1471-2334-2-9
- 10 Scottish Medical Journal. 1977;22(4):310-313
- 11 Zeitschrift fur Haut- und Geschlechtskrankheiten, 01 Sep 1967, 42(18):749-754
- 12 Annals of the New York Academy of Sciences, 141: 506-516
- 13 Br Med J. 1970 Dec 26;4(5738):776–780
- 14 Br Med J. 1974 Jun 8;2(5918):526-7
- 15 Med Clin (Barc). 1992 Feb 22;98(7):245-9
- 16 N Z Med J. 1981 Nov 25;94(696):384-6
- 17 Journal of Biological Chemistry, Volume 278, Issue 35, 33185-33193
- 18 Aust J Biol Sci. 1977 Apr;30(1-2):141-53
- 20, 21 The Forgotten Side of Medicine, October 20, 2024
- 22 Curr Ther Res Clin Exp. 1964 Feb:6:134-5
- 23 Ann N Y Acad Sci. 1967 Mar 15;141(1):261-72
- 24 J. Pharm. Sci., 58: 836-839
- 25, 26 Annals of the New York Academy of Sciences, (1967), 141(1), 451-456
- 27 Oftalmol Zh. 1976;31(3):168-70
- 28, 37 Amazon, DMSO: Nature’s Healer
- 29, 31, 35, 39, 60, 68, 70 The Forgotten Side of Medicine, December 29, 2024
- 30 Ann N Y Acad Sci. 1967 Mar 15;141(1):572-85
- 32 Amazon, DMSO: The True Story of a Remarkable Pain-Killing Drug
- 33, 51 Amazon, The DMSO Handbook for Doctors
- 34 Mikrobiolohichnyi Zhurnal, 01 Nov 1973, 35(6):766-769
- 36 Kazan Medical Journal 1983, Volume 64, No. 6, Pages 434-435
- 38 World Health Organization, Tuberculosis, October 29, 2024
- 40 Zh Ushn Nos Gorl Bolezn. 1969 Nov-Dec;29(6):68-71
- 41 Pediatriia, 01 Jan 1980, (9):24-25
- 42 Problemy Tuberkuleza, 01 Jan 1991, (3):34-36
- 43 Intern Med. 1993 May;32(5):359-64
- 44 American Journal of Physiology, Gastrointestinal and Liver Physiology, Volume 276, Issue 2, February 1999, Pages G485-G490
- 45 J Infect Dis. 1983 Nov;148(5):844-54
- 46 Wikipedia, Shigellosis
- 47 Equine Vet J. 2008 Jun;40(4):358-63
- 48 Eur Respir J Suppl. 1990 Oct:11:482s-484s
- 49 Research Laboratory of General Reanimatology of the USSR Academy of Medical Sciences, Issue: Vol 63, No 5 (1982)
- 50 Anesteziol Reanimatol. 1984 Jul-Aug:(4):38-40
- 52 Ann N Y Acad Sci. 1975 Jan 27:243:460-7
- 53 Benghazi University Medical Journal, September 2020, 1(4), doi: 10.37376/benunivmedj.v1i4.2474
- 54 The Forgotten Side of Medicine, November 17, 2024
- 55 Khirurgiia (Mosk). 1974 Oct:(10):53-7
- 56 Vrachebnoe Delo, 01 Oct 1975, (10):96-98
- 57 Antibiotiki, 01 Feb 1981, 26(2):102-104
- 58 Kaf. Infekts. Bol., Med. Inst., Kiev, Volume 7, 1978, Pages 146-148 (Archived)
- 59 Vrach Delo. 1987 Feb:(2):113-5
- 61 Vestnik Khirurgii Imeni I. I. Grekova, 01 Jan 1976, 116(1):90-92
- 62 Vestnik Khirurgii Imeni I. I. Grekova, 01 Feb 1980, 124(2):135-138
- 63 Vestnik Khirurgii Imeni I. I. Grekova, 01 Sep 1978, 121(9):88-90
- 64 Vestnik Khirurgii Imeni I. I. Grekova, 01 Aug 1979, 123(8):133-136
- 65 Vestnik Khirurgii Imeni I. I. Grekova, 01 Jul 1981, 127(7):94-96
- 66 Vestn Khir Im I I Grek. 1986 Mar;136(3):51-3
- 67 Urol Nefrol (Mosk). 1986 Nov-Dec:(6):50-2
- 69 Arch Intern Med. 1969;124(6):748–753
- 71 Klin Khir (1962). 1978 Dec:(12):34-7
- 72 Khirurgiia (Mosk). 1984 Apr:(4):19-22
- 73 Vestnik Khirurgii Imeni I. I. Grekova, 01 Feb 1985, 134(2):63-64
- 74 Klin Khir (1962). 1984 Jan:(1):49-52
- 75 Klinicheskaia Khirurgiia, 01 Jan 1990, (1):35-36
- 76 Klin Khir (1962). 1988:(1):1-3
- 77 Diagnostic Microbiology and Infectious Disease, Volume 75, Issue 1, January 2013, Pages 60-63
- 78 Antimicrob Agents Chemother. 1986 Oct;30(4):617-8
- 79 Sabouraudia: Journal of Medical and Veterinary Mycology, 9(1), 43–49
- 80 Vestn Dermatol Venerol. 1974 May;48(5):45-9
- 81 JAMA. 1965 Sep 13:193:923-8 CONCL. doi: 10.1001/jama.1965.03090110061015
- 82 Stomatologiia (Mosk). 1977 May-Jun;56(3):25-7
- 83 J Am Vet Med Assoc. 1997 Jul 15;211(2):199-203
- 84 The Korean Journal of Parasitology 2017; 55(1): 81-84
- 85 J S C Med Assoc. 1966 Jul;62(7):265-6
- 86 Arch Dermatol. 1966;94(5):643-645
- 87 Vrachebnoe Delo, 01 Jun 1984, (6):76-77
Autopsies Confirm COVID Jab Hazards in Youth
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2023/02/23/autopsies-confirm-covid-jab-hazards-in-youth.aspx
The original Mercola article may not remain on the original site, but I will endeavor to keep it on this site as long as I deem it to be appropriate.
Analysis by Dr. Joseph Mercola Fact Checked February 23, 2023

STORY AT-A-GLANCE
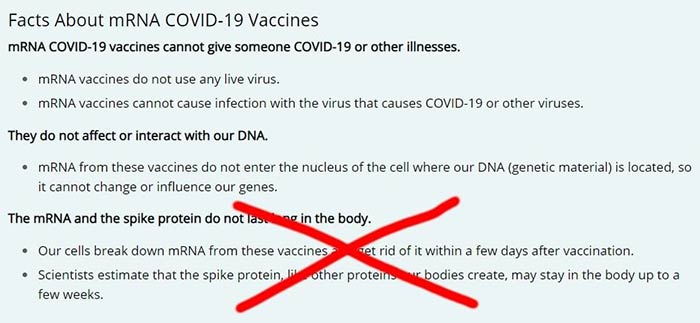
- When the COVID shots were first introduced, the U.S. Centers for Disease Control and Prevention made several claims about them that have since been proven completely false, including the claim that the mRNA would remain in the injection site, and that both the mRNA and resulting spike protein would rapidly be eliminated from your body
- The mRNA goes everywhere and can remain intact for a month of more. Ditto for the spike protein your cells produce
- Spike protein has been found in the brains of people with encephalitis (brain inflammation) and in jab-induced shingles lesions. Both mRNA and spike protein have been found in lymph nodes more than 60 days post-jab. Full-length mRNA has also been shown to circulate in people’s blood for up to 28 days post-injection, and it’s been detected in breastmilk
- Research shows the primary difference between those who developed symptoms of myocarditis and those who didn’t was that symptomatic patients had markedly elevated levels of full-length spike protein unbound by antibodies in their plasma. Those who remained asymptomatic had no free spike protein in their blood. This would suggest that free-floating spike protein is a problem
- Autopsies of two teenage boys found dead in their beds three and four days after their second dose of Pfizer concluded jab-induced heart damage was to blame. The myocarditis described in these instances did not have the typical histopathology of myocarditis. Instead, both cases resemble catecholamine-induced injury, similar to the cytokine storm experienced in severe SARS-CoV-2 infection
When the COVID shots were first introduced, the U.S. Centers for Disease Control and Prevention made several claims about them that have since been proven completely false.
They claimed the mRNA in the shot would remain in and only affect the cells around the injection site. They also claimed the mRNA and resulting spike protein wouldn’t last long in your body. The mRNA, they said, would vanish within “a few days,” and the spike protein produced by your cells would be eliminated within “a few weeks.”
As it turns out, virtually every cell in your body is exposed to the mRNA and can remain intact for a month or more. Ditto for the spike protein your cells produce. Spike protein has been found in the brains of people with encephalitis (brain inflammation)1 and in jab-induced shingles lesions.2 It can bioaccumulate in several organs,3,4 including reproductive organs.
Both mRNA and spike protein have been found in lymph nodes more than 60 days post-jab.5 Full-length mRNA has also been shown to circulate in people’s blood6 for up to 28 days post-injection,7 and it’s been detected in breastmilk.8
In early August 2022, the CDC suddenly deleted those statements from its website — probably because they realized their lies were catching up to them. The cleanup effort was caught, however. Disclose TV exposed the deletion on its Twitter account,9 with an archived link showing the CDC’s original webpage.
Free Spike Protein Linked to Jab-Induced Myocarditis
From the get-go, physicians and scientists warned that the SARS-CoV-2 spike protein was the most toxic part of the virus, and hence making your cells produce it for an undetermined amount of time could be an unmitigated disaster. Their warnings were “debunked” and censored, but mounting evidence now proves their concerns were valid — and should have been shared to prevent the loss of life.
We now have case reports, studies and autopsy findings showing that people suffering from post-jab myocarditis have mRNA-induced spike proteins in their hearts and blood.
Interestingly, a January 2023 study10 in the journal Circulation found “extensive antibody profiling and T-cell responses” both in those who developed post-jab myocarditis and asymptomatic jabbed controls.
The primary difference between those who developed symptoms of myocarditis and those who didn’t was that symptomatic patients had “markedly elevated levels of full-length spike protein unbound by antibodies” in their plasma. Those who remained asymptomatic had no free spike protein in their blood. This would suggest that free-floating spike protein is a profoundly serious problem. As concluded by the authors:
“Immunoprofiling of vaccinated adolescents and young adults revealed that the mRNA vaccine-induced immune responses did not differ between individuals who developed myocarditis and individuals who did not.
However, free spike antigen was detected in the blood of adolescents and young adults who developed post-mRNA vaccine myocarditis, advancing insight into its potential underlying cause.”
Autopsy Reports Confirm Jab-Related Myocarditis
mRNA programming the heart cells to produce spike protein is also profoundly bad news. A case report11 published in September 2022 describes the case of a 55-year-old man who died from acute myocardial infarction and lymphocytic myocarditis four months after a dose of Pfizer. As his first dose, he’d received the AstraZeneca shot. According to the author:
“SARS-CoV-2 Spike protein, but not nucleocapsid protein was sporadically detected in vessel walls by immunohistochemical assay … These findings indicate that myocarditis, as well as thrombo-embolic events following injection of spike-inducing gene-based vaccines, are causally associated with a injurious immunological response to the encoded agent.
Because of the fact that the immune response to a first gene-based vaccination is very low in comparison with the immune response to the second vaccination, the found adverse events has rather to be attributed to the mRNA-based second vaccination as to the initial vector-based one.”
A Korean report12 published in July 2021 describes the case of a 22-year-old healthy male military recruit who developed chest pain five days after his first Pfizer dose and died just seven hours later. The primary cause of death was determined to be “myocarditis, causally associated with the BNT162b2 vaccine.” Here, the primary autopsy findings were:
- Myocarditis predominantly involving the atrial wall, with neutrophil and histiocyte predominance
- Noninflammatory single-cell necrosis
- Diffuse contraction band necrosis (CBN) throughout the myocardium, predominantly in the left ventricle. CBN is a type of uncontrolled cell death that can occur during reperfusion (reoxygenation). Basically, the tissue is damaged when the blood returns into the tissue after a period of ischemia or lack of oxygen
- Enlargement of the heart
The myocarditis was determined to be “histologically different from viral or immune-mediated myocarditis in that the inflammatory infiltrates were predominantly neutrophils and histiocytes, rather than lymphocytes.”
Neutrophils are a type of white blood cells that act as your immune system’s first line of defense. Histocytes are immune cells normally found in many areas of your body, but when they move into tissues where they don’t belong, such as your heart, they damage those tissues, which is what appears to have happened here.
A November 2022 paper describing the autopsy findings from five people who “died suddenly” within seven days of their COVID jabs concluded that most of the deaths were caused by acute arrhythmogenic cardiac failure. “Thus, myocarditis can be a potentially lethal complication following mRNA-based anti-SARS-CoV-2 vaccination,” the authors concluded.
Download this Article Before it Disappears
Teenage Boys Killed by COVID Jab
A report13 detailing the autopsies of two teenage boys found dead in their beds three and four days after their second dose of Pfizer also concluded jab-induced heart damage was to blame.
The autopsies primarily sought to determine whether the myocarditis described in these instances had the typical histopathology of myocarditis. It did not. Instead, both cases more closely resembled a catecholamine-induced injury. As described by the authors:
“The myocardial injury seen in these postvaccine hearts is different from typical myocarditis and has an appearance most closely resembling a catecholamine-mediated stress (toxic) cardiomyopathy …
The microscopic findings are not the alterations seen with typical myocarditis. This suggest a role for cytokine storm, which may occur with an excessive inflammatory response, as there also is a feedback loop between catecholamines and cytokines.”
As in the case of the Korean military man, both boys had evidence of CBN which, as explained earlier, is cell death that typically occurs during reperfusion, when blood flow temporarily ceases and then returns. The actual damage occurs when blood reenters the tissue. As described in this report:14
“Both teenage boys had similar clinical presentations with no obvious cardiac symptoms. Their histopathology did not demonstrate a typical myocarditis. In those instances, one sees lymphocytic (or giant cell) infiltrates with adjacent myocyte necrosis; changes such as hypereosinophilic myocytes and contraction bands are absent.
In these two postvaccination instances, there are areas of contraction bands and hypereosinophilic myocytes distinct from the inflammation.
This injury pattern is instead similar to what is seen in the myocardium of patients who are clinically diagnosed with Takotsubo, toxic, or stress cardiomyopathy, which is a temporary myocardial injury that can develop in patients with extreme physical, chemical, or sometimes emotional stressors.
Stress cardiomyopathy is a catecholamine-mediated ischemic process seen in high catecholamine states in the absence of coronary artery disease or spasm. It has also been called ‘neurogenic myocardial injury’ and ‘broken heart syndrome.’
Surges in catecholamines may have several triggers (fight/flight response, adrenal pathology, etc). Proposed mechanisms for catecholamine-mediated stunning in stress cardiomyopathy include epicardial spasm, microvascular dysfunction, hyperdynamic contractility with midventricular or outflow tract obstruction, and direct effects of catecholamines on cardiomyocytes.
Catecholamine-mediated myocardial stunning may be due to direct myocyte injury, as elevated catecholamines decrease the viability of myocytes through cyclic adenosine monophosphate–mediated calcium overload.
Catecholamines also are a potential source of oxygen-derived free radicals, which can interfere with sodium and calcium transporters, possibly resulting in myocyte dysfunction through increased transsarcolemmal calcium influx and cellular calcium overload …
We suspect that the acute cardiac changes seen in these two boys are the result of epinephrine-mediated effects on cardiomyocytes … This postvaccine reaction may represent an overly exuberant immune response, with the myocardial injury mediated by similar immune mechanisms to those described with SARS-CoV-2 and multisystem inflammatory syndrome cytokine storms …
These two clinical histories support the etiology of the acute myocardial injury as a primary factor, not a secondary agonal or postresuscitative artifact … Cytokine storm has been described with an excessive and uncontrolled inflammatory response, and there is a feedback loop between catecholamines and cytokines.
Clinical complications may include cardiac compromise, respiratory distress, and hypercoagulation. The myocardial injury seen in these postvaccine hearts has a similar histologic appearance to catecholamine-mediated stress cardiomyopathy and severe SARS-CoV-2 infection, including myocarditis, which is associated with cytokine release syndrome.
Recognition that these instances are different from typical myocarditis and that cytokine storm has a known feedback loop with catecholamines may help guide screening, diagnosis, and therapy.”
Myocarditis — New Top Cause of Death Among COVID-Jabbed
Have our federal health agencies destroyed the hearts of tens of thousands of young Americans by pushing and mandating these shots? The preponderance of evidence suggests this is most likely. A recent survey15 by Steve Kirsch suggests myocarditis and sudden death are now two of the top causes of death in the U.S., but only among those who got the COVID jab.
In early October 2022, Florida Surgeon General Dr. Joseph Ladapo issued updated COVID jab guidance,16,17 recommending men between the ages of 18 and 39 abstain from getting any more shots, as data show an 84% increase in heart-related death within 28 days of injection. Men over the age of 60 have a 10% increased risk of cardiac-related death within 28 days.
The mass injection campaign has already shaved more than three years off the U.S. life expectancy, and in the future, I predict we’ll see even further drops as jab-related heart problems continue to take their toll.
As reported by Edward Dowd in his book “Cause Unknown: The Epidemic of Sudden Deaths in 2021 and 2022,” excess death rates began to skyrocket in the 26- to 41-year-old group shortly after the COVID jabs were rolled out.18 Between February 2021 and March 2022 alone, millennials experienced the equivalent of a Vietnam war with more than 60,000 excess deaths. Mass injection is the only thing that can account for this sudden rise in mortality in this age group.
When young people are killed off en masse like this, the overall life expectancy will drop rather massively, and if the systemic damage caused by these shots continue for years on end, we could be facing a rather noticeable depopulation event.
Sudden deaths among high-performance athletes have also skyrocketed by nearly 1,700%,19 and COVID jab mandates is the only novel factor that’s come into play. Approximately 1,148 professional and amateur athletes suffered a lethal cardiac event in 2021 and 2022, giving us an annual average death rate of 574 for those years.20,21,22,23,24,25 Meanwhile, the historical annual average has been between 2826 and 29.27
When young people are killed off en masse like this, the overall life expectancy will drop rather massively, and if the systemic damage caused by these shots continues for years on end, we could be facing a rather noticeable depopulation event.
Resources for Those Injured by the COVID Jab
If you got one or more jabs and suffered an injury, first and foremost, never ever take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your body.
The same goes for anyone who has taken one or more COVID jabs and had the good fortune of not experiencing debilitating side effects. Your health may still be impacted long-term, so don’t take any more shots.
When it comes to treatment, there are still more questions than answers, and most doctors are beyond clueless about what to do — in part because they never agreed or bothered to provide early treatment for COVID and therefore don’t understand how different medicines and supplements impact the spike protein.
So far, it seems like many of the treatments that worked against severe COVID-19 infection also help ameliorate adverse effects from the jab. This makes sense, as the toxic, most damaging part of the virus is the spike protein, and that’s what your whole body is producing if you got the jab.
So, eliminating the spike protein your body is continuously producing is a primary task to prevent and/or address post-jab injuries. The two preferred remedies for this are hydroxychloroquine and ivermectin. Both of these drugs bind and thereby facilitate the removal of spike protein.
The Front Line COVID-19 Critical Care Alliance (FLCCC) has developed a post-vaccine treatment protocol called I-RECOVER. Since the protocol is continuously updated as more data become available, your best bet is to download the latest version straight from the FLCCC website at covid19criticalcare.com28 (hyperlink to the correct page provided above).
The World Health Council has also published lists of remedies that can help inhibit, neutralize and eliminate spike protein. Natural substances that prevent spike protein from binding to your cells include Prunella vulgaris, pine needle tea, emodin, neem and dandelion extract.
Spike protein neutralizers, which prevent the spike from damaging cells, include N-acetylcysteine (NAC), glutathione, fennel tea, star anise tea, pine needle tea, St. John’s wort, comfrey tea and vitamin C. A March 2022 review paper29 suggests combating the neurotoxic effects of the spike protein using luteolin and quercetin.
Time-restricted eating (TRE) and/or sauna therapy can also help eliminate toxic proteins by stimulating autophagy. Several additional detox remedies can be found in “World Council for Health Reveals Spike Protein Detox.”
Other Helpful Treatments and Remedies
Other treatments and remedies that may be helpful for COVID jab injuries include:
• Hyperbaric oxygen therapy, especially in cases involving stroke, heart attack, autoimmune diseases and/or neurodegenerative disorders. To learn more, see “Hyperbaric Therapy — A Vastly Underused Treatment Modality.”
• Lower your omega-6 intake. Linoleic acid is consumed in amounts ten times of ideal in well over 95% of the population and contributes to massive oxidative stress that impairs your immune response. Seed oils and processed foods need to be diligently avoided. You can review my previous post for more information.
• Pharmaceutical grade methylene blue, which improves mitochondrial respiration and aid in mitochondrial repair. It’s actually the parent molecule for hydroxychloroquine. A dose of 15 to 80 milligrams a day could go a long way toward resolving some of the fatigue many suffer post-jab.
It may also be helpful in acute strokes. The primary contraindication is if you have a G6PD deficiency (a hereditary genetic condition), in which case you should not use methylene blue at all. To learn more, see “The Surprising Health Benefits of Methylene Blue.”
• Near-infrared light, as it triggers production of melatonin in your mitochondria30 where you need it most. By mopping up reactive oxygen species, it too helps improve mitochondrial function and repair. Natural sunlight is 54.3% infrared radiation,31 so this treatment is available for free. For more information, see “What You Need to Know About Melatonin.”
• Lumbrokinase and serrapeptidase are both fibrinolytic enzymes taken on an empty stomach one hour before or two hours after to help reduce the risk of blood clots.
- 1 Vaccines 2022; 10(10): 1651
- 2 Journal of Cutaneious Immunology and Allergy August 25, 2022; 6(1): 18-23
- 3 SARS-CoV-2 mRNA Vaccine BNT162 Biodistribution Study
- 4 Trialsitenews May 28, 2021
- 5 Cell 2022; 185: 1025-1040
- 6 Clinical Infectious Diseases February 15, 2022; 74(4): 715-718
- 7 Rheumatology & Autoimmunity January 17, 2023; 131(3): 128-132
- 8 JAMA Pediatrics 2022; 176(12): 1268-1270
- 9 Twitter Disclose.tv August 13, 2022
- 10 Circulation January 4, 2023; 0
- 11 Preprints.org September 5, 2022
- 12 Journal of Korean Medical Science 2021; 36(40): e286
- 13, 14 Archives of Pathology & Laboratory Medicine February 14, 2022; 146(8): 925-929
- 15 Steve Kirsch Substack December 27, 2022
- 16 Florida Health October 7, 2022
- 17 WFLA.com October 10, 2022, Updated October 11, 2022
- 18 Conservative Woman January 3, 2023
- 19, 26 The Expose November 23, 2022
- 20 Journal of Scandinavian Immunology Letter to the Editor December 17, 2022
- 21 Twitter Liz Wheeler January 3, 2023
- 22 Twitter Liz Wheeler January 3, 2023, Archived
- 23 The Expose List of Athlete Deaths, April 2022
- 24 Epoch Times January 4, 2023 (Archived)
- 25 Good Sciencing Athlete Deaths List
- 27 Rumble Peter McCullough Interview January 4, 2023
- 28 Covid19criticalcare.com
- 29 Molecular Neurobiology March 2022; 59(3): 1850-1861
- 30 Physiology February 5, 2020 DOI: 10.1152/physiol.00034.2019
- 31 Journal of Photochemistry and Photobiology February 2016; 155: 78-85
Shingles Activation Associated With COVID Jab
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2023/01/04/covid-vaccine-shingles.aspx
The original Mercola article may not remain on the original site, but I will endeavor to keep it on this site as long as I deem it to be appropriate.
Analysis by Dr. Joseph Mercola Fact Checked January 04, 2023
STORY AT-A-GLANCE
- According to a recent case study, persistent post-jab shingles was associated with the presence of COVID jab spike protein in the affected skin. The researchers speculate that the COVID jab may induce persistent shingles reactivation by perturbing the immune system
- Another study details the cases of six patients with autoimmune inflammatory rheumatic diseases who developed shingles shortly after their Pfizer jabs. None of the healthy controls developed shingles post-jab
- A systematic review also concluded that the COVID jab increases the risk of shingles reactivation if you’ve had it before or have known risk factors for it
- The COVID shots suppress your innate immune system by inhibiting the type-1 interferon pathway, which is the first-stage response to all viral infections. Type-1 interferon also keeps latent viruses in check, so if your interferon pathway is suppressed, latent viruses can start to emerge
- Type 1 interferon is suppressed by the jab because it responds to viral RNA, and viral RNA is not present in the COVID shot. The RNA is modified to look like human RNA, so the interferon pathway is not triggered
According to a recent case study1 published in the Journal of Cutaneous Immunology and Allergy, persistent post-jab shingles, aka herpes zoster, an infection caused by the varicella zoster virus, was associated with the presence of COVID jab spike protein in the affected skin. As explained by the authors:2
“Since the campaign of vaccination against COVID-19 was started, a wide variety of cutaneous adverse effects after vaccination has been documented worldwide. Varicella zoster virus (VZV) reactivation was reportedly the most frequent cutaneous reaction in men after administration of mRNA COVID-19 vaccines, especially BNT162b2.
A patient, who had persistent skin lesions after BNT162b2 vaccination for … over 3 months, was investigated for VZV virus and any involvement of vaccine-derived spike protein … Strikingly, the vaccine-encoded spike protein of the COVID-19 virus was expressed in the vesicular keratinocytes and endothelial cells in the dermis.”
COVID Jab Impairs Your Immune Function
The researchers speculate that the COVID jab may induce persistent shingles reactivation by “perturbing the immune system.” How your immune system is perturbed by the COVID shots is the topic of MIT researcher Stephanie Seneff’s paper3 “Innate Immune Suppression by SARS-CoV-2 mRNA Vaccinations: The Role of G-quadruplexes, Exosomes and MicroRNAs,” co-written with Drs. Peter McCullough, Greg Nigh and Anthony Kyriakopoulos.
In it, they describe how the COVID shots suppress your innate immune system by inhibiting the type-1 interferon pathway, which is the first-stage response to all viral infections.
When a cell is invaded by a virus, it releases type-1 interferon alpha and beta. Both of these molecules act as signaling molecules that tell the cell it’s been infected. That, in turn, launches the immune response and gets it going early in the viral infection.
Type-1 interferon also keeps latent viruses in check, so if your interferon pathway is suppressed, latent viruses can start to emerge. The U.S. Vaccine Adverse Event Reporting System (VAERS) database reveals many who have been jabbed report these kinds of infections. Regulators in the European Union are also warning that repeat COVID shots can weaken overall immunity.4
How is type-1 interferon suppressed by the jab? It’s suppressed because type-1 interferon responds to viral RNA, and viral RNA is not present in the COVID shot. The RNA is modified to look like human RNA, so the interferon pathway is not triggered. Worse, the interferon pathway is actively suppressed by the microRNA in the shot, which limits your ability to fight off all viruses. It also opens the door for latent viruses to reactivate.
In the case study above, the patient had received one dose of Pfizer’s mRNA shot 13 days before the shingles outbreak and a second dose eight days after, causing the researchers to suspect there was an association between the outbreak and the shots.
COVID Jab and Shingles in the Immunocompromised
Similarly, a study5,6 published in April 2021 detailed the cases of six patients with autoimmune inflammatory rheumatic diseases who developed shingles shortly after their Pfizer jabs.
“The safety profile of mRNA-based vaccines in patients with autoimmune inflammatory rheumatic diseases (AIIRD) is unknown,” the authors noted.7 “The objective of this report is to raise awareness of reactivation of herpes zoster (HZ) following the BNT16b2 mRNA vaccination in patients with AIIRD.”
The study found herpes infection occurred in 1.2% of AIIRD patients who got the shot (six out of 491), compared to none among controls. Five of them developed shingles for the first time in their life a short time after their first dose of Pfizer. One got it after her second dose.
As noted by the authors, immunosuppressed patients, including patients with AIIRD, have been prioritized for the COVID jab, even though immunosuppressed patients were excluded from the clinical trials. The fact that 1.2% of immunocompromised patients developed shingles, whereas none of the healthy controls suffered this fate, shows you just how important it is not to confine clinical trials to the healthiest among us.
Pathogenic Mechanisms
As for the mechanisms, the researchers offered the following:8
“Potential mechanisms that might explain the pathogenetic link between mRNA-COVID19 vaccination and HZ reactivation are related to stimulation of innate immunity through toll-like receptors (TLRs) 3,7 by mRNA-based vaccines. TLR signaling has been implicated during reactivation of herpesviruses, a process essential for these viruses to maintain themselves in the host.
Defects in TLR expression in patients suffering from diseases caused directly by herpesvirus infection highlight the importance of these signaling pathways during infection and eventual disease progression.
The vaccine stimulates induction of type I INFs [type 1 interferon] and potent inflammatory cytokines, which instigate T and B immune responses but may negatively affect antigen expression potentially contributing to HZ reactivation.”
COVID Jab Raises Risk of Shingles Reactivation
A systematic review9 published in November 2021 also concluded that the COVID jab increases the risk of shingles reactivation if you’ve had it before or have known risk factors for it. Fifty-four cases involving 27 men and 27 women had been reported at the time and were included in the review. As noted by the authors:10
“There were cases with known risk factors for herpes zoster, which included age more than 50 years (n = 36), immunological disorders (n = 10), chronic disease (n = 25), metabolic disorder (n = 13), malignancy (n = 4), and psychiatric disorder (n = 2).
The mean (SD) period between development of herpes zoster and COVID-19 vaccination was 7.64 (6.92) days. Majority of the cases were from the high-income and/or middle-income countries. 86.27% of the cases of HZ were reported due to mRNA vaccine. Thirty-six patients 36/45 (80%) developed herpes zoster following the priming dose of COVID-19 vaccine among those who received mRNA vaccine.
We could not establish definite link but there may be possible association between COVID-19 vaccine and shingles. Large-scale studies may help to understand the cause-effect relationship.”
Shingles Reports in VAERS
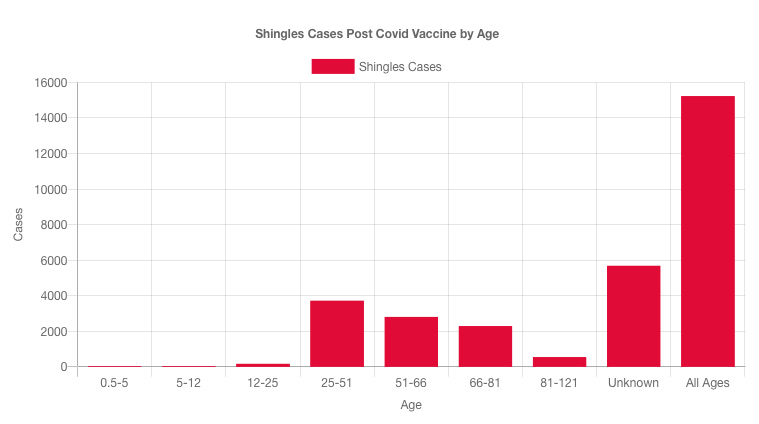
Looking at VAERS, as of December 16, 2022, there were 15,225 reports of shingles after the COVID jab.11 Most cases (for which age are given) have occurred in younger individuals between the ages of 25 and 51, which is younger than normal. There are even 170 cases in 12- to 25-year-olds.
The Pfizer shot has more than double the number of shingles reports associated with it than Moderna, and there are more than twice the number of reports from women than men.
Can VAERS Data Demonstrate Causality?
One person who has taken a strong stance against the claim that VAERS data cannot tell us anything about causation is Steve Kirsch, executive director of the COVID-19 Early Treatment Fund. In the video “Vaccine Secrets: COVID Crisis,”12 he argues that VAERS can indeed be used to determine causality.
It’s important to realize that the idea that VAERS cannot show causality is part of how and why the CDC can claim none of the deaths is attributable to the COVID shot. Kirsch argues that this premise is in fact false, and that causation can be determined using VAERS’ data.
To prove his point, Kirsch gives the following analogy: Suppose you give a two-dose vaccine. After the first dose, nothing happens, but after the second dose, people die within 24 hours of a deep vein thrombosis (DVT).
When you look at the VAERS data, what you would find is no reports associated with the first dose, and a rash of deaths after the second dose, all within the same timeframe and with the same cause of death.
According to the CDC, you cannot ascribe any causality at all from that. To them, it’s just random chance that everyone died after the second dose, and from the same condition, and not the first dose or from another condition.
Kirsch argues that causality can indeed be identified from this kind of data. It’s very difficult to come up with another explanation for why people — many who are young, in perfect health with no predisposing conditions — die exactly 24 hours after their second dose. It’s even difficult to come up with another explanation for people who do have underlying conditions.
For example, is it reasonable to assume that people with, say, undiagnosed heart conditions, would die from DVT exactly 24 hours after getting a second dose of vaccine? Or that people with undiagnosed diabetes would die from DVT exactly 24 hours after their second dose?
Why not after the first dose, or two months after the second dose, or any other random number of hours or days, or for other random cause of death? Why would people randomly die of the same condition at the exact same time, repeatedly?
At bare minimum, as an early warning system, VAERS is designed to flag potential causation. It’s by looking for repeated patterns of side effects that you would begin to identify a potentially problematic vaccine.
Once a pattern is identified — and there’s no denying death within 24 hours to one week is a pattern seen for the COVID shots — an investigation should be launched. But no such investigation has been launched into the COVID jabs. Clear-cut patterns are simply ignored.
Ignoring Warning Signs Does Not Make the Shots Safe
As an early warning system, VAERS is performing as intended, despite severe underreporting (the CDC even published a paper in which they admitted COVID jab adverse effects in children are underreported by a factor of 6.513). It’s the follow-up that’s lacking.
But lack of investigation and follow-up is not evidence that the shots can’t cause problems, one of which is reactivation of latent viruses such as shingles. While I don’t believe these shots are beneficial for anyone, if you have a history of latent infection, be aware that the shot may cause a flare-up.
Also be aware that having a compromised immune system will render you more prone not only to COVID-19 but also any number of other viral and bacterial infections, plus chronic diseases such as cancer.
- 1, 2 Journal of Cutaneous Immunology and Allergy August 25, 2022
- 3 Food Chem Toxicol June 2022; 164: 113008
- 4 Business Standard January 12, 2022
- 5, 7 Rheumatology October 2021; 60(SI): 190-195
- 6 Channel 7 News April 20, 2021
- 8 Rheumatology October 2021; 60(SI): 190-195, Discussion
- 9, 10 J. Cosmet Dermatol November 2021; 20(11): 3350-3361
- 11 OpenVAERS Shingles Reports as of December 16, 2022
- 12 Lew Rockwell October 11, 2021
- 13 Steve Kirsch Substack January 6, 2022