Chemotherapy
now browsing by category
Unlocking DMSO — The Forgotten Molecule That Makes Drugs Work Better, Safer, and Faster
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2025/07/04/unlocking-dmso.aspx
Analysis by A Midwestern Doctor July 04, 2025

Story at-a-glance
- DMSO is an “umbrella remedy” capable of treating a wide range of challenging ailments due to its combination of therapeutic properties (e.g., reducing inflammation, improving circulation, and reviving dying cells)
- One of DMSO’s unique properties is its ability to enter through the skin and carry anything it dissolves with it as it rapidly travels throughout the body, greatly enhancing the potency and viability of many pharmaceutical drugs
- Because of this, numerous preparations over the years have combined DMSO with a commonly used medication, and in many cases, demonstrated safety and efficacy of the combination to drug regulators
- Some of these DMSO combination therapies are able to treat challenging illnesses, such as significant musculoskeletal injuries, antibiotic resistant infections, persistent fungal and viral infections, chemotherapy resistant cancers, and chronic pain
- More creative DMSO combinations (which can be produced at home) have been frequently used to successfully treat many challenging conditions (e.g., tinnitus, a wide range of eye issues, cancers, and uncomfortable scars)
DMSO is a remarkable naturally occurring substance that (provided it’s used correctly1) safely and rapidly improves a variety of conditions medicine struggles with — particularly chronic pain. For example, thousands of studies show DMSO treats a wide range of:
• Injuries such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
• Strokes, paralysis, many neurological disorders (e.g., Down syndrome and dementia), and numerous circulatory disorders (e.g., Raynaud’s, varicose veins, or hemorrhoids), which were discussed here.
• Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which was discussed here.
• Many autoimmune, protein, and contractile disorders, such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
• Head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
• Internal organ diseases such as pancreatitis, infertility, liver cirrhosis, and endometriosis (discussed here).
• A wide range of skin conditions, such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
• Many challenging infections, such as shingles, herpes, chronic ear or dental infections, and osteomyelitis (discussed here).
• Cancers and many complications from the illness and its treatments (discussed here).
In turn, since I started this series, it struck a chord, and I have received over 2,000 reports of remarkable responses to DMSO, and many readers have had for a variety of “incurable conditions.”
This begs an obvious question — if a substance capable of doing all of that exists, why does almost no one know about it? Simply put, like many other promising therapies, it fell victim to a pernicious campaign by the FDA, which kept it away from America despite decades of scientific research, congressional protest, and thousands of people pleading for the FDA to reconsider its actions. Consider for example, this 60 minutes program about DMSO that aired on March 23, 1980:
Understanding DMSO’s Combination Potential
DMSO’s effectiveness in treating a wide range of illnesses stems from its unique and diverse properties, many of which appear to target the root causes of disease — such as enhancing parasympathetic activity, improving circulation, regenerating senescent cells, providing potent anti-inflammatory effects, and blocking pain conduction. Sadly, despite hundreds of studies demonstrating these promising characteristics, the FDA has refused to recognize all but one property of DMSO.
In pharmacology, DMSO is often referred to as a “vehicle” that helps other drugs get into the body. Because of this, while DMSO only has one approved (intravesical) use in the United States, a variety of drugs are on the market that use DMSO as a “vehicle” to transport them in the body.
In short, when DMSO is given alone, it is “unsafe” and “unproven” but when combined with a patentable drug, it suddenly becomes “safe and effective.” Likewise, in package inserts, DMSO is typically described as a safe and inert ingredient (despite it often being the primary “active ingredient”).
DMSO’s ability to serve as a drug delivery system is due to its being a potent solvent with a variety of unique properties.
• Membrane permeability — DMSO will pass through biological membranes without damaging them, which is extremely unusual.2 This property is believed to be due to its exchange and interchange with water in biological membranes.3 In addition to not harming the skin, when tested with other substances that could enter the brain, DMSO was not observed to alter the cells lining the blood-brain barrier or the brain tissue.4
• Rapid distribution — Once it contacts the skin, DMSO rapidly spreads throughout the body. Within an hour of being applied to the skin, it can be found within the bones and teeth.5 Interestingly, DMSO does not penetrate tooth enamel or nails, which may explain why certain conditions affecting these structures require different approaches.6
• Solvent properties — DMSO is a highly potent solvent that can dissolve a wide range of polar and non-polar substances (and hence is sometimes used to solubilize other drug products). If a substance is dissolved within DMSO, DMSO can typically bring it into the body. While a few other substances can also serve as vehicles, DMSO is the most potent in pharmacology (e.g., DMSO is more effective than propylene glycol at delivering topical steroids into the body7).
• Enhanced circulation and cellular transport — Beyond simply transporting substances into the body, DMSO also greatly increases circulation. By taking the place of water (as it is small, can form hydrogen bonds, and is relatively polar) while being both fat and water soluble, it changes the permeability of the cell membrane, allowing new things to enter the cell and waste products to leave the cells.
As a result, DMSO is able to both spread what it transports throughout the body and significantly enhance the body’s innate ability to circulate what has already been absorbed (including to previously inaccessible areas).
This combination of properties enables the topical administration of drugs that would normally require injection, and in many cases, can significantly increase their potency because it penetrates deep regions of the body that pharmaceuticals typically have difficulty entering, or because it bypasses the cellular barriers that normally exclude foreign substances.
In turn, lower doses of drugs can frequently be used (reducing their toxicity) because they become more potent, and because DMSO combinations can be locally applied to bring a drug to a target region, rather than taking a standard oral dose that raises the entire body’s target concentration.
• Specialized DMSO pharmaceuticals — These properties allow well established drugs to be combined with DMSO. For example, NSAIDs (which are also used to treat pain and musculoskeletal injuries) have a variety of side effects when consumed orally (e.g., fatal NSAIDs gastric bleeds killed over 16,000 Americans in 19998). However, when combined with DMSO, NSAIDs can be applied topically to the site of injury, thereby avoiding the risks of oral NSAID consumption.
One FDA-approved drug (Pennsaid) does just that, and in clinical trials, it was found to have minimal systemic toxicity. DMSO significantly enhances the efficacy of diclofenac (Pennsaid’s NSAID) while exhibiting much lower toxicity compared to oral diclofenac.9,10,11,12
Many other FDA approved pharmaceutical products utilizing DMSO further demonstrate its therapeutic versatility:
◦Mekinist, a targeted cancer therapy, uses DMSO to stabilize the drug and enhance its water solubility, possibly increasing tumor penetration.13
◦Prochymal, a stem cell product for preventing tissue rejection, uses 10% DMSO to preserve stem cells, as do many other stem cell products.14
◦Onyx, a liquid injected into blood vessels to seal leaks, uses DMSO to dissolve the polymer so it remains liquid until reaching problem areas. DMSO is chosen because it’s a uniquely safe substance capable of this function.15
◦Viadur is a non-degradable implant for prostate cancer containing Lupron dissolved in DMSO, designed to slowly release Lupron over a year.16 DMSO is essential because Lupron is otherwise difficult to dissolve, and DMSO preserves its stability while being nontoxic.
Note: Lupron is an incredibly toxic hormone eliminating drug used for prostate cancer which was adopted by urologists due to it being incredibly lucrative (which then led to it being repurposed for many other areas of medicine such as gynecology and blocking puberty in transgender children).
Critical Considerations
DMSO’s function as a vehicle and potentiator has enabled a variety of innovations for common medical therapies (e.g., pain-killers, antibiotics, and chemotherapy), which has inspired many others to experiment with these combinations. However, for anyone planning to do this, it is critical to understand the safety precautions that must accompany using DMSO in this manner.
• Contamination risk — One of the major risks of DMSO is its potential to exacerbate the effects of a toxic substance already present in the skin, so it is crucial to clean the skin thoroughly before applying DMSO. The original investigator of DMSO learned this lesson the hard way when researching toxic pesticides.17
[Herschler] wanted to investigate whether certain highly toxic pesticides were soluble in DMSO. The researcher felt how soluble they were when he sprayed some of the solution onto his skin. DMSO transported the poison into the body within minutes. The poison worked: Herschler temporarily suffered from impaired consciousness and shortness of breath.
Remarkably, despite the immense potential harm, serious incidents are extremely rare, suggesting either that users are consistently careful about cleaning skin prior to DMSO applications or that the actual risk is limited to highly toxic substances.
• Potentiation effects — Many agents become significantly more potent when mixed with DMSO, and in a few reports made rare side effects typically seen at higher doses manifest (something which has occasionally been reported with the more toxic antibiotics like fluoroquinolones or certain chemotherapy drugs).
With natural substances, this is generally not problematic (as their potency and toxicity are typically much less than pharmaceuticals). Still, it remains a real consideration (although I have not come across any reports of this injuring someone).
• Size limitations — While DMSO can draw things inside the body, it can only do so for smaller molecules, with the size limit thought to be around 500 daltons (although there are numerous examples of larger drugs also being transported).
For this reason, DMSO tends to work well as a vehicle for individual drugs or chemicals but not larger proteins (e.g., peptides). Likewise, pathogenic organisms are far too big for DMSO to transport, so areas of application do not need to be disinfected prior to application.
Note: Below the skin, the transportation limit is much higher (e.g., evidence suggests DMSO can bring molecules larger than 70,000 Da through the blood-brain barrier, opening even wider possibilities for intravenous applications).18
• Purity requirements — When making DMSO combinations, it’s essential to obtain pure ingredients, as many pharmaceutical and supplement preparations contain multiple ingredients beyond the primary active compound
Note: One of DMSO’s most promising combinations is with a common dye (hematoxylin) as this combination selectively targets tumors with no toxicity to normal tissue and has remarkable efficacy against a wide range of cancers. Unfortunately, hematoxylin is often mixed with heavy metals (to better stain tissues), illustrating the need to ensure pure substances with DMSO.
• Leaching — As a solvent, DMSO can leach toxic chemicals (e.g., those added to the surfaces of plastics) and hence later bring them into the body. For this reason, it is advisable to avoid storing DMSO in plastic that is not DMSO resistant and to avoid mixing or preparing DMSO with plastic tools.
In most cases, DMSO only leaches plastic at concentrations about 20%, so if DMSO is diluted before putting it in contact with plastic many of these issues can be avoided. Likewise, many DMSO compatible materials exist for preparing DMSO combinations — all of which is discussed further here.
Note: Most implanted medical devices are not at risk of DMSO leaching them as it dilutes far below 20% by the time it reaches them and can contact their plastic components. The one exception are within dental implants, and for that reason, DMSO mouthwashes must always be sufficiently diluted.

Save This Article for Later – Get the PDF Now
DMSO Drug Interactions
Given DMSO’s ability to potentiate pharmaceuticals, a critical question arises: is it safe to take alongside other drugs? The answer is nuanced:
• What we know — Most pharmaceutical interactions, unfortunately, have not been studied. Fortunately (particularly since over 61% of Americans are on at least one medication19), significant reactions are rarely reported.
Generally speaking, the risk for potentiation is stronger the closer they are taken together (particularly when mixed together in an IV infusion) so it is generally advised to space DMSO and a pharmaceutical by at least two hours, and in the case of more toxic ones (e.g., fluoroquinolones and certain chemotherapies) by at least two days.
Note: DMSO can also mitigate many pharmaceutical toxicities, such as gentamicin’s kidney toxicity20 or many injuries caused by chemotherapy.
Most of the research into DMSO’s interactions was conducted during the initial trials in the 1960s, where it was discovered DMSO significantly potentiated alcohol and also potentiated barbiturates, corticosteroids, insulin, digitalis, nitroglycerin, quinidine sulfate, and chemotherapy21 (leading to lower doses sometimes being needed).
Since then, DMSO has also been observed to potentiate certain opioids (e.g., morphine patches), NSAIDs, anticonvulsants (e.g., gabapentin), and certain sedatives (e.g., trazodone). Users typically do not report potentiation of anticoagulants; however, as a serious risk might exist, it is advisable to monitor your coagulation parameters when using both concurrently.
Note: Insulin potentiation is hypothesized to result from DMSO’s protein refolding capacity restoring the functionality of insulin receptors.22
Conversely, DMSO has also been observed to reverse the effects of Botox, likely by neutralizing the toxin induced paralysis.
Therapeutic Synergies
Over the years, many remarkable pharmaceutical DMSO combinations have been developed for a wide range of medical applications. These include:
• Antibiotics — Antibiotic resistance is a major problem in medicine. However, when combined with DMSO, many organisms that are chronic and debilitating or life threatening (e.g., tuberculosis) lose their resistance to antibiotics.
DMSO also makes it possible to reach infections such as those within the bones that are normally difficult to reach and otherwise require maintaining very high blood concentrations of the drugs to ensure this result. Finally, in many cases (both for cost and to protect the gut microbiome) being able to topically apply an oral or IV antibiotic can be immensely advantageous (e.g., for mastitis or Lyme disease).
• Antifungals — Fungal infections are often located in areas that topical and oral antibiotics have difficulty penetrating. However, research shows combining an antifungal with topical DMSO can reach those infections and there are many reports of multiyear fungal infections quickly resolving from this combination.
• Herpes and shingles — Some of the most potent antiviral medications have difficulty penetrating through a lesion to where the virus resides. However, once combined with DMSO they do, and many clinical trials have proven the efficacy of these antiviral combinations.
• Corticosteroids — For issues within the body, steroids (which have significant systemic toxicity) must be injected or taken orally. When combined with DMSO, this is often no longer needed, and as DMSO potentiates steroids, much lower and far less toxic doses can be taken to address an autoimmune or musculoskeletal issue.
• Chemotherapy — By potentiating chemotherapy, DMSO has been proven to cure chemotherapy resistant cancers, and in many cases does so with much lower doses being needed.
Recently, owing to the emerging popularity of using ivermectin for treating cancer (which sometimes produces spectacular results but typically fits best as a complementary therapy), physicians have begun combining ivermectin with DMSO into a paste and topically applying it over tumors. While data is limited, this appears to consistently work, and sometimes produces dramatic responses like this one James Miller MD recently shared with me:
“I had a patient with a thoracic sarcoma that was debilitatingly painful with growth through a couple of ribs and metastases to his skull base that became basically pain free after 2 days of topical DMSO-ivermectin. At his 2.5 week follow up, he was completely pain free and had returned to playing racketball.”
Note: Nothing comparable to do this can be done with conventional cancer options (and given the severity of that situation, what would be used is also fairly toxic).
Conclusion
As so many things can be combined with DMSO, the incredible things we’ve seen so far are only the tip of the iceberg, and only the most preliminary (but highly encouraging) data exists on many of them, as there is so much to research. For example, DMSO combinations have been shown to effectively treat a wide range of eye issues (e.g., eye strain, macular degeneration, glaucoma, and cataracts), traumatic injuries (e.g., whiplash) tinnitus, uncomfortable scars, neuropathic pain and Lyme disease.
Likewise, DMSO combination therapies are not restricted to pharmaceuticals, and as such, over the years, the DMSO community has discovered hundreds of incredible natural DMSO combinations that revolutionize natural medicine.
Stanley Jacob, the father of DMSO who devoted his career to advancing the science of it, was driven by the recognition DMSO was not a new drug, but rather, like penicillin, a new therapeutic principle which redefined how medicine could be practiced. Fortunately, due to an extraordinary confluence of circumstances, we have now arrived in an era where it is at last (after more than a century) no longer possible to suppress natural healing methods.
People around the world are at last awakening to the Forgotten Sides of Medicine and the realization that the ways to find the cures we need is not “more research” but rather rediscovering what was already found (but not possible to profit off of). This is an incredibly exciting time and I am immensely grateful to be part of it with you.
Author’s Note: This is an abridged version of a longer article about DMSO combination therapies which goes into greater detail on the points mentioned here, many of the other combinations not covered (e.g., for tinnitus or vision loss), and provides guidance for preparing the combination therapies. That article, along with resources and protocols for obtaining and using DMSO can be read here.
A Note from Dr. Mercola About the Author
A Midwestern Doctor (AMD) is a board-certified physician from the Midwest and a longtime reader of Mercola.com. I appreciate AMD’s exceptional insight on a wide range of topics and am grateful to share it. I also respect AMD’s desire to remain anonymous since AMD is still on the front lines treating patients. To find more of AMD’s work, be sure to check out The Forgotten Side of Medicine on Substack.
- 1, 17 A Midwestern Doctor, June 21, 2025
- 2, 6 Annals of the New York Academy of Sciences, 243: 7-19
- 3 International Journal of Molecular Veterinary Research, 2013, Vol. 3, No. 6 (Archived)
- 4 Science. 1982 Jul 9;217(4555):164-6
- 5 Annals of the New York Academy of Sciences, 141: 85-95
- 7 Annals of the New York Academy of Sciences, 141: 428-436
- 8 Cleveland Clinic Journal of Medicine Volume 66, Number 9, October 1999
- 9 JAMA Internal Medicine | Vol. 164, No. 18
- 10 Current Medical Research and Opinion, 32(2), 241–250
- 11 Pain. 2009 Jun;143(3):238-245
- 12 The Journal of Rheumatology 2006; 33:3
- 13 Wikipedia, Trametinib
- 14 Wikipedia, Prochymal
- 15 Medtronic, OnyxTM Liquid Embolic System
- 16 Urology. 2003 Dec 22;62(6 Suppl 1):36-42
- 18 Science, 9 Jul 1982, Vol. 217, Issue 4555, pp. 164-166
- 19 kff.org, October 04, 2024
- 20 Universidad Dr. José Matías Delgado, 2012 (Archived)
- 21 Annals of the New York Academy of Sciences, 141: 532-550
- 22 A Midwestern Doctor, September 15, 2024
Chemotherapy creates toxic chain reaction in healthy cells, new research reveals
Reproduced from original article:
https://www.naturalhealth365.com/chemotherapy-creates-toxic-chain-reaction-in-healthy-cells-new-research-reveals.html
by: April 25, 2025
 (NaturalHealth365) When cancer patients receive chemotherapy, they’re rarely told about the biological “time bomb” being activated inside them – one that continues exploding long after treatment ends.
(NaturalHealth365) When cancer patients receive chemotherapy, they’re rarely told about the biological “time bomb” being activated inside them – one that continues exploding long after treatment ends.
A new study published in BJC Reports has unmasked the hidden mechanism behind chemotherapy’s devastating long-term effects, revealing a truth far different from what oncologists have been telling patients.
The toxic cascade your doctor won’t discuss
When chemotherapy kills cells, it triggers something alarming: dying cells release dangerous fragments called “cell-free chromatin particles” (cfChPs) into the bloodstream. Unlike normal cell death, chemotherapy creates a tsunami of these toxic particles that overwhelm your body’s cleanup systems.
These particles don’t just disappear – they actively penetrate healthy cells throughout your body, damaging DNA and activating inflammatory pathways in organs far from the original tumor site. This explains why so many chemotherapy patients develop “secondary cancers,” cognitive impairment, heart damage, and immune dysfunction years after treatment.
Even more concerning, this damage accumulates with each treatment cycle. Every chemotherapy session creates a new flood of these toxic particles, which can remain active in the body for months, creating a compounding toxic burden that conventional medicine completely ignores.
The statistics they don’t share
The damage from chemotherapy’s toxic particles is extensive:
- Secondary leukemias appear in up to 6.8% of patients receiving certain chemotherapy agents
- Cardiac damage occurs in up to 26% of patients receiving anthracycline chemotherapy
- Permanent nerve damage affects 30-40% of patients receiving platinum-based chemotherapy
- Cognitive impairment (“chemo brain”) affects up to 75% of chemotherapy recipients
Until now, these side effects were attributed simply to direct drug toxicity. The discovery that many are caused by this secondary wave of cfChP damage – damage that continues long after treatment ends – should transform how we approach cancer care.
Yet this crucial information remains largely buried while patients suffer unnecessarily.
The solution Western medicine ignores
The most revolutionary aspect of this research is discovering that natural compounds can effectively neutralize these toxic particles, potentially preventing much of chemotherapy’s collateral damage.
Researchers identified a combination of resveratrol (found in grape skins) and copper that demonstrated a remarkable ability to bind to cfChPs and prevent them from entering healthy cells. Unlike pharmaceutical interventions, this natural approach works with the body’s own detoxification systems to neutralize the threat without causing additional side effects.
Other natural agents showing promise include:
- Quercetin: This flavonoid found in apples and onions helps stabilize cell membranes, making them more resistant to cfChP penetration.
- N-acetylcysteine: This powerful antioxidant helps replenish glutathione, your body’s primary defense against toxic compounds.
- Medicinal mushrooms: Compounds in reishi and turkey tail help modulate the immune response to cfChPs and support normal cell repair.
What makes these natural approaches especially valuable is that they don’t appear to interfere with chemotherapy’s anti-cancer effects – they specifically target the secondary damage while allowing the chemotherapy to still attack cancer cells.
What every cancer patient needs to know
If you or a loved one is facing chemotherapy, these findings highlight critical protective steps:
- Work with an integrative oncologist who understands both conventional treatments and evidence-based natural approaches.
- Time your protective agents properly – research suggests taking them in the days before and after treatment, not during chemotherapy itself.
- Support your cellular repair systems with compounds like sulforaphane (from broccoli sprouts) and ellagic acid (from pomegranates).
- Enhance elimination pathways through hydration, lymphatic drainage techniques, and targeted nutritional support.
- Monitor for delayed effects, particularly in vulnerable organs like the heart, brain, and bone marrow.
The bottom line: Knowing what to do can protect your health
The revelation that chemotherapy creates a cascade of damage through toxic cfChPs represents both a warning and an opportunity. The warning is clear: conventional cancer treatments may be causing far more extensive and long-lasting damage than patients realize.
The opportunity is equally significant: Much of this damage may be preventable with proper understanding and appropriate supportive strategies. Natural compounds represent a new frontier in protective oncology – one that focuses not just on killing cancer cells, but on preserving the health of the person fighting cancer.
Are you looking to protect your cells from cancer and the toxic effects of conventional treatments? Discover natural, science-backed strategies to support your body’s natural defenses against cellular damage.
Sources for this article include:
Chemotherapy Spreading Cancer
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2024/02/08/chemotherapy-spreading-cancer.aspx
The original Mercola article may not remain on the original site, but I will endeavor to keep it on this site as long as I deem it to be appropriate.
Analysis by Dr. Joseph Mercola February 08, 2024

STORY AT-A-GLANCE
- Preoperative chemotherapy may increase the likelihood of metastasis in breast cancer cases by increasing what are known as “tumor microenvironments of metastasis”
- When mice with breast cancer were given preoperative chemotherapy, it altered the tumor microenvironment in ways that made them more conducive to cancer spread
- In mice, chemotherapy treatment doubled the number of cancer cells in the bloodstream and lungs compared to mice that did not receive the treatment
- In 20 human patients who received common chemotherapy drugs, the tumor microenvironments also became more favorable to cancer spread
Dr. Lee Cowden says most people don’t die from cancer; they die from the side effects of treatment. While the “war against cancer” is moving toward more personalized and so-called “precision medicine” treatments, the old standby model of “cut, poison and burn,” via surgery, chemotherapy and radiation, is still widely used and regarded as the standard of care for many cancer cases.
One of the major problems with chemotherapy is its indiscriminate toxicity, which poisons your body systemically in an attempt to knock out cancer cells. There have long been signs that this model has fatal flaws and may cause more harm than good. In the case of the breast cancer chemotherapy drug Tamoxifen, for instance, patients must trade one risk for another, as while it may reduce breast cancer, it more than doubles women’s risk of uterine cancer.1
Serious, sometimes-fatal side effects (or more aptly, simply effects) of chemotherapy are common, as are serious unforeseen effects that may make your cancer prognosis worse instead of better.
Writing in the journal Science Translational Medicine, researchers from the Albert Einstein College of Medicine revealed that giving chemotherapy prior to surgery for breast cancer may promote disease metastasis, or the growth and spread of cancer to other areas of the body.2 This, in turn, greatly increases a woman’s risk of dying from the disease.
Chemotherapy May Make Breast Cancer More Aggressive and Likely to Spread
Preoperative chemotherapy, known as neoadjuvant chemotherapy, is often offered to women because it may help shrink tumors, which increases the likelihood that women will receive lumpectomy surgery instead of a full mastectomy. After performing tests on mice and human tissue, however, the researchers found that doing so may increase the likelihood of metastasis by increasing what are known as “tumor microenvironments of metastasis.” As Stat News explained:3
“Called ‘tumor microenvironments of metastasis,’ these on-ramps are sites on blood vessels that special immune cells flock to. If the immune cells hook up with a tumor cell, they usher it into a blood vessel like a Lyft picking up a passenger. Since blood vessels are the highways to distant organs, the result is metastasis, or the spread of cancer to far-flung sites.”
When mice with breast cancer or given human breast tumors were given the chemotherapy, it altered the tumor microenvironment in ways that made them more conducive to cancer spread, including, Stat reported:4
- Increasing the number of immune cells that transport cancer cells into blood vessels
- Making blood vessels more permeable to cancer cells
- Making tumor cells more mobile
In mice, chemotherapy treatment doubled the number of cancer cells in the bloodstream and lungs compared to mice that did not receive the treatment. Further, in 20 human patients who received common chemotherapy drugs, the tumor microenvironments also became more favorable to cancer spread. As The Telegraph noted:
“It is thought the toxic medication switches on a repair mechanism in the body which ultimately allows tumors to grow back stronger. It also increases the number of ‘doorways’ on blood vessels which allow cancer to spread throughout the body.”5
Further, researchers wrote in a 2012 Journal of Clinical Oncology editorial, “Unfortunately, neoadjuvant chemotherapy does not seem to improve overall survival, as demonstrated in the National Surgical Adjuvant Breast and Bowel Project (NSABP) B18 trial, among others.”6 This means women may be trading a potential increased risk of cancer metastasis for a treatment that doesn’t even improve their chances of survival.
It’s Been Known for Years That Chemotherapy Can Trigger Tumor Growth
While the news that chemotherapy may encourage cancer spread may sound surprising, it’s not a new discovery. In 2012, researchers found chemotherapy for prostate cancer caused DNA damage in healthy cells and caused them to secrete more of a protein called WNT16B, which boosts tumor growth and may encourage cancer cells to develop resistance to treatment.
“WNT16B, when secreted, would interact with nearby tumor cells and cause them to grow, invade and, importantly, resist subsequent therapy,” study co-author Dr. Peter Nelson, of the Fred Hutchinson Cancer Research Center, told AFP News.7
In the journal Nature Medicine, the researchers further noted, “The expression of WNT16B in the prostate tumor microenvironment attenuated the effects of cytotoxic chemotherapy in vivo, promoting tumor cell survival and disease progression”8 and “… [D]amage responses in benign cells … may directly contribute to enhanced tumor growth kinetics.”9
While research continues to reveal that chemotherapy’s effects are wide-reaching and devastating to healthy cells, it’s also been shown — at least as far back as 2004 — that “chemotherapy only makes a minor contribution to cancer survival.”10 A Clinical Oncology study found that in terms of five-year survival rates in adult cancer cases, chemotherapy has an average five-year survival success rate of just 2.3% in Australia and 2.1% in the U.S.11
Separate research revealed that out of nearly 2,000 patients receiving chemotherapy, 161 deaths occurred within 30 days of the treatment. Nearly 8% of them were classified as related to the chemotherapy (and another nearly 16% were unclassified due to insufficient information).12
Further, as mentioned, chemotherapy can increase the risk of subsequent cancer, such as therapy-related acute myeloid leukemia (tAML), “a rare but highly fatal complication of cytotoxic chemotherapy.” Researchers noted that tAML cases occur nearly five times more often in adults treated with chemotherapy than they do in the general population.13
Download this Article Before it Disappears
Conventional Oncologists Aren’t Likely to Explain the Many Options for Treatment
Upon receiving a cancer diagnosis, many people assume their only options for treatment are chemotherapy, surgery or radiation. Only you and your health care team can make the decision on how to best pursue treatment, but you should know that conventional providers are unlikely to think outside the box.
Oncology is the only specialty in medicine that is allowed and even encouraged to sell drugs at massive profits — typically in excess of 50% — and cancer drugs are, as a general category, the most expensive medications in all of medicine to begin with. Oncologists actually get a commission for the chemotherapy drugs they sell, and with that type of incentive, it’s nearly impossible to imagine them actively seeking other alternatives.
Oncologists are further constrained by the “standard of care” prescribed by oncology medical boards and the drug industry. If they go against the established standard of care, they’re susceptible to having their license reprimanded or even taken away. As a result, patients are typically forced to go it alone if they don’t want to go the conventional route, which is unfortunate because there are many promising alternative treatments.
Understanding Your Options for Cancer Treatment
A comprehensive natural cancer-fighting approach would be to make your body as healthy as possible, using detoxification, strategies to boost your immune function, dietary changes and other targeted therapies depending on your needs. For instance, Annie Brandt — a 16-year cancer survivor and author of “The Healing Platform: Build Your Own Cure!” — states products that are helpful against metastatic cancer cells include:
| Berberine / metformin | Intravenous vitamin C | Sulforaphane (cruciferous vegetables) |
| Curcumin (turmeric) | Broccoli sprouts | Glucoraphanin |
| Myrosinase | Essiac tea | Burdock root |
| Slippery elm | Rhubarb | Sheep sorrel |
| Fermented soy | Fish oil | Modified citrus pectin (PectaSol-C) |
| Heparin |
The point is that there are many anticancer strategies overlooked by conventional medicine. Many of them even work in addition to conventional treatment. For instance, vitamin C in combination with nutritional ketosis and fasting prior to administering chemotherapy radically improve the effectiveness of chemotherapy.
Oncologists in Turkey, who aren’t under the same U.S. restrictions, are also using a stacked ketogenic treatment protocol that is showing shocking remissions in many stage 4 cancer patients. The treatment protocol at ChemoThermia Oncology Center in Turkey includes:
- Metabolically supported chemotherapy (applying chemotherapy with a variety of interventions to support its effectiveness)
- Hyperthermia
- Hyperbaric oxygen therapy
- Glycolysis inhibitors, especially 2-deoxyglucose (2-DG) and dichloroacetate (DCA)
- Ketogenic diet with phytopharmaceutical supplements
At the center, all oncology patients are put on a ketogenic diet, which creates metabolic stress on the cancer cells. Then, prior to administering the chemo, the patient will do a 14-hour fast, which further increases the metabolic stress on the cancer cells.
The patients will typically have a blood glucose level around 80 milligrams per deciliter (mg/dL) at this point. They then apply glycolysis inhibitors to inhibit the glycolysis pathway in the cancer cells, which creates a terrific amount of metabolic stress, as the cancer cells are already starved of glucose.
Insulin is then applied to lower the blood glucose levels to around 50 or 60 mg/dL, to cause mild hypoglycemia. At that point, chemotherapy is applied, often at a far lower dose than would otherwise be used, thereby lowering the risk of side effects.
In the days following chemotherapy, hyperthermia and hyperbaric oxygen therapy are applied, plus a daily infusion of glycolysis inhibitor therapies with high-dose vitamin C (50 grams) and dimethyl sulfoxide (DMSO). A sampling of other targeted therapies covered in Brandt’s book are below.
| Poly-MVA, a colloidal mineral complex that crosses the blood-brain barrier and helps renourish your body and brain at the cellular level. It also helps replace nutrients lost during chemotherapeutic and radiological treatments. |
| AvéULTRA (Metatrol), a fermented wheat germ product. |
| Selenium, vitamin D and iodine, as most cancer patients are low in these three nutrients. Since I do regular sauna therapy, I take 200 micrograms of SelenoExcell each day. (You tend to excrete selenium when sweating.) Selenium increases glutathione, an important metabolic antioxidant necessary for detoxification. It also catalyzes the conversion of thyroid hormone T4 to T3, so it can be beneficial if you have thyroid problems. |
| Modified citrus pectin (MCP) has been shown to reverse cancer and stop metastatic cancer. Brandt recommends the brand ecoNugenics, as this is the one that has been scientifically studied and verified to work. |
| Colloidal silver is a nontoxic, broad-spectrum antimicrobial therapy with no known toxicity and no known mechanism for acquired resistance. |
| Salicinium, a plant-based extract that inhibits production of nagalase — an enzyme produced by cancer cells — while simultaneously stimulating innate immune cells. |
So as mentioned, there are many promising avenues to target cancer. Even if you’re working with a conventional oncologist, the ChemoThermia Oncology Center has published protocols your oncologist could make use of, regardless of where you live. If your oncologist isn’t willing to integrate these alternative strategies into your care regimen, you may want to consider finding a new doctor.
- 1 International Journal of Gynecological Cancer August 16, 2007 (Archived)
- 2 Science Translational Medicine July 5, 2017
- 3, 4 Stat News July 10, 2017
- 5 The Telegraph July 5, 2017
- 6 Journal of Clinical Oncology May 2012
- 7, 9 AFP Relax News August 6, 2012 (Archived)
- 8 Nat Med. 2012 Sep;18(9):1359-68
- 10, 11 Clin Oncol (R Coll Radiol). 2004 Dec;16(8):549-60
- 12 Br J Cancer. 2006 Dec 18; 95(12): 1632–1636
- 13 Blood. 2013 Apr 11; 121(15): 2996–3004
WARNING: Breast cancer treatment can increase risk of heart failure
Reproduced from original article:
https://www.naturalhealth365.com/breast-cancer-chemotherapy-2504.html
by: November 29, 2023
 (NaturalHealth365) Highly-toxic chemotherapy sessions (along with radiation) are often used to treat breast cancer. However, evidence is mounting that those who survive are left with debilitating health problems, including brittle bones and cognitive issues like “chemo brain.”
(NaturalHealth365) Highly-toxic chemotherapy sessions (along with radiation) are often used to treat breast cancer. However, evidence is mounting that those who survive are left with debilitating health problems, including brittle bones and cognitive issues like “chemo brain.”
And now, new research shows that chemotherapy can lead to a higher probability of heart failure. Tragically, this aligns with prior research indicating a threefold higher likelihood of heart failure in breast cancer and lymphoma survivors. This elevated risk emerges as early as one year post-cancer diagnosis.
Breast cancer patients deserve better treatment
Mayo Clinic researchers monitored 900 breast cancer and lymphoma patients, along with 1,550 individuals without cancer, from 1985 to 2010 to track incidents of heart failure. Those with cancer were found to be three times more prone to experience heart failure within five years of diagnosis.
Even after two decades, they remained twice as likely to develop heart failure compared to cancer patients who hadn’t undergone chemotherapy. The risk was notably influenced by both high doses of chemotherapy and the presence of diabetes.
Chemotherapy actually INEFFECTIVE for most cancer types
The toxic side effects of chemotherapy are nothing new for most readers of NaturalHealth365. In fact, one of our contributors, the late Nicholas Gonzalez, MD, did all he could to raise awareness about the dangers of chemotherapy and his more sensible approach to dealing with all types of cancer, known as “The Gonzalez Protocol.”
The truth – exposed by Dr. Gonzalez – is that chemotherapy was originally derived from leftover World War II nerve gas chemicals – yes, that’s right – chemicals used against the enemy in warfare. If that doesn’t tell you all you need to know about chemotherapy, not much else will.
However, Dr. Gonzalez also provided evidence that chemotherapy is not effective for most cancer types, including breast cancer. The shocking truth is that it is only somewhat effective for bloodborne cancers like lymphoma and leukemia, not cancers of the organs.
Better ways to treat cancer are available today
Despite his tragic passing, Dr. Gonzalez’s message lives on: Chemotherapy is NOT your only option when it comes to eliminating the threat of cancer. This message of hope lives on thanks to the work of hundreds of holistic physicians promoting the value of good (organic) nutrition and detoxification as the foundation for a full recovery.
To steer clear of the adverse effects of harsh cancer treatments, consult with a seasoned healthcare provider who aligns with your preference for healthy lifestyle habits. Address dental concerns, such as the extraction of infected teeth treated with root canals, and incorporate high-quality nutritional supplements.
Embrace detoxification protocols, including far infared sauna therapy, fresh juices, glutathione, and possibly coffee enemas. Explore the benefits of medicinal herbs, mushrooms, and a range of other holistic approaches with your healthcare professional and/or health coach.
The bottom line: never underestimate the ability of the body to heal itself – when given what it needs to thrive.
Editor’s note: Discover the many natural ways to stop cancer cell growth, own the Stop Cancer Docu-Class created by NaturalHealth365 Programs.
Sources for this article include:
Cut, Poison, Burn — Is Radiation Treatment on the Way Out?
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2023/09/19/radiation-treatment.aspx
The original Mercola article may not remain on the original site, but I will endeavor to keep it on this site as long as I deem it to be appropriate.
Analysis by Dr. Joseph Mercola Fact Checked September 19, 2023
STORY AT-A-GLANCE
- Under the cut, poison, burn model, cancer remains a top killer worldwide; by 2040, it’s expected that 29.5 million new cancer cases will occur each year, along with 16.4 million cancer-related deaths
- Researchers are realizing that in some cases, radiation may be causing more harm than good — and leaving it out of cancer treatment entirely may not change the outcome
- A 2022 study found no difference in outcomes among those who received radioactive iodine after surgery for thyroid cancer and those who did not after three years
- In many low-risk cancer cases, omitting radiation from treatment did not have an effect on survival rates
- Radiation therapy also increases the risk of solid tumors, including lung, thyroid, bone, pancreatic, stomach, liver and colorectal cancers, which often develop 10 years or more after the treatment; recent research also suggests cancer risks from low-dose radiation exposure may be underestimated
Modern medicine’s go-to strategies for cancer treatment are archaic, based on the “cut, poison, burn” model — or surgery, chemotherapy and radiation. The idea of using toxic therapies to destroy tumors should represent a last resort, if used at all, not a first-line treatment.
By their very nature, chemotherapy and radiation have devastating effects on the human body and the healing process, leaving providers to walk a fine line between issuing a dose strong enough to destroy the tumor without killing the patient. Often, basic supportive strategies designed to target cancer’s root causes — and boost the body’s capacity to heal — are ignored in favor of radiation and all of its significant side effects.
“The conventional approach seems to follow the logic ‘destroy to heal,’ and I just don’t know where that really occurs in nature outside conventional cancer treatment. Healing has to be your focus and goal to achieve healing. You have to heal to heal,” Dr. Nathan Goodyear explained in our 2022 interview.1
Under the cut, poison, burn model, cancer remains a top killer worldwide. By 2040, it’s expected that 29.5 million new cancer cases will occur each year, along with 16.4 million cancer-related deaths.2 The tide may be slowly turning, however, with some in the field suggesting radiation treatment for cancer may be fading out.3
Radiation for Cancer — A Focus on Omission or De-Escalation
Speaking with STAT, Corey Speers, vice chair of radiation oncology at the University Hospitals Seidman Cancer Center and Case Western Reserve University, stated that radiation may be on the way out in many cases of cancer treatment:4
“We are in an era of radiation omission or de-escalation. Radiation is perhaps one of the most precise and most effective cancer therapies we have, so it will always play an important role in cancer management, but there are situations now on an individual patient basis where radiation may not be needed.”
The fact is, using radiation to kill cancer cells without causing extreme side effects in the patient is not an exact science. “The balance has always been the question — is reducing the intensity of treatment going to impact the long-term effectiveness? People didn’t know what to do starting off, so they decided to treat people until they had to stop — until they couldn’t take it anymore,” Abram Recht, a radiation oncologist at Beth Israel Deaconess Medical Center, told STAT.5
Now, however, researchers are realizing that in some cases, radiation may be causing more harm than good — and leaving it out of treatment entirely may not change the outcome.
“There’s also been this long history of trying to reduce the morbidity of radiation in different ways, and the big thing that people think about is the best way to reduce morbidity is to not give it at all,” Recht said.6 For example, in certain low-risk cases involving lymphoma,7 thyroid cancer8 and others, omitting radiation from treatment did not have an effect on survival rates.9
If You Don’t Need It, ‘You Shouldn’t Receive It’
Radiation is often offered as a failsafe to patients after surgery, to catch any cancer cells that may be left behind. But only recently have scientists begun to show that outcomes are often the same whether a patient receives radiation or not. This seems to be the case for low-risk cases of thyroid cancer.
After surgery, “It’s almost a given that once patients have their thyroid taken out, they get radioactive iodine,” David Cooper, an endocrinologist at the Johns Hopkins University School of Medicine, told STAT. “Recently, people have been wondering whether it really does what it’s supposed to, whether its potential harms are worth the potential benefits.”10
The radioactive iodine is taken in by thyroid cells and thyroid cancer cells alike, resulting in cell death. But a 2022 study published in the New England Journal of Medicine found no difference in outcomes among those who received the radioactive iodine and those who did not after three years. In other words, receiving radiation therapy is useless in these cases:11
“In patients with low-risk thyroid cancer undergoing thyroidectomy, a follow-up strategy that did not involve the use of radioiodine was noninferior to an ablation strategy with radioiodine regarding the occurrence of functional, structural, and biologic events at 3 years.”
In 2012, scientist and oncologist Dr. Sophie Leboulleux and colleagues conducted a study that found a much smaller dose of radiation than was the norm at that time could manage low-risk thyroid cancer, noting, “The administration of the smallest possible amount of radioiodine would improve care.”12
This led the team to conduct the 2022 New England Journal of Medicine Study. Leboulleux told STAT, “For low-risk [thyroid cancer] we felt there might not be any need for it. So we decided to do another study to see if radioiodine therapy was even useful.” Indeed, it turned out it was not. “Radiation is just one more worry for a patient. Once you know that you don’t need it, I don’t think you should receive it,” she said.13
Download this Article Before it Disappears
Radiation Treatment Can Cause Cancer
Radiation treatment should be avoided as much as possible, since it’s toxic by nature. The side effects vary depending on the area of the body being treated. Along with fatigue, which is a near universal side effect of radiation therapy, you may experience any of the following:14
| Hair loss | Memory problems | Nausea and vomiting |
| Skin changes | Headaches | Blurry vision |
| Swelling and tenderness | Throat problems, including trouble swallowing | Cough |
| Shortness of breath | Mouth problems | Taste changes |
| Less active thyroid gland | Diarrhea | Sexual problems |
| Fertility problems | Urinary and bladder problems |
There’s also a risk that radiation therapy will lead to the development of a second cancer. Radiation exposure is a risk factor for most types of leukemia, along with myelodysplastic syndrome, a type of bone marrow cancer that may turn into leukemia.
Radiation therapy also increases the risk of solid tumors, including lung, thyroid, bone, pancreatic, stomach, liver and colorectal cancers, which often develop 10 years or more after the treatment. In one study of 52,613 patients who received radiation therapy, an increased risk of second cancer was found even after 40 years compared to the general population.15
“Radiotherapy has been considered as a double-edged sword as it has a well-established role in the management of solid cancers but unfortunately it is likely to induce cancers years after the treatment,” researchers explained in Radiation Oncology Journal.16 Chemotherapy is also linked with the development of second cancers.17
Susan Wadia-Ells, Ph.D., was inspired to write “Busting Breast Cancer: Five Simple Steps to Keep Breast Cancer Out of Your Body” after losing several friends to recurrent metastatic breast cancer, meaning cancer that was “successfully treated” at an early stage, only to later return as a terminal stage or metastatic disease.18
If you are going to submit your body to radiation, it’s best to protect your body with molecular hydrogen, probably two tablets twice a day for three days before and after the treatment. It would also be helpful to make sure you are taking 50 mg of niacinamide three times a day and methylene blue 50 mg once a day for a few days before and after the treatment.
Even Low-Dose Radiation Exposure Increases Cancer Deaths
Efforts to eliminate radiation therapy altogether may be necessary to protect cancer patients from subsequent cancers. A study that investigated workers in the nuclear industry in France, the U.K. and the U.S., who are exposed to low doses of ionizing radiation over longer periods of time, found an increased risk of cancer mortality.19
A linear increase in the relative rate of cancer was found with increasing radiation exposure, and risk of solid cancers increased by 52% for every unit of radiation each worker absorbed.20 The cancer risks from low-dose radiation exposure may, in fact, be underestimated. According to the study:21
“For the purposes of radiation protection, people often assume that low dose rate exposures pose less carcinogenic hazard than the high dose rate exposures experienced by the Japanese atomic bomb survivors … Our study does not find evidence of reduced risk per unit dose for solid cancer among workers typically exposed to radiation at low dose rates.”
Dr. Nasha Winters is a naturopathic physician who specializes in supporting patients with cancer. She also trains clinicians and consults with those treating cancer patients. Winter is the coauthor of “Mistletoe and the Emerging Future of Integrative Oncology,” and is herself a cancer survivor, so this topic is close to her heart.
Mistletoe Can Be Used as an Adjunct for All Cancers
According to Winters, mistletoe is likely to be useful as an adjunct therapy for all cancers, and she, along with several other doctors, has been training physicians on how to use mistletoe for several years now.
“One of our physicians has been using mistletoe for 45 years in his practice, and what we’ve seen clinically, and what the research suggests, is that this therapy, it has always been about using it with others. It plays very well with others.
It was never really developed to be a standalone therapy, though believe me, we’ve seen impact with that as well. And it has virtually no contraindications with any of our standard of care therapies. So, we can literally inject this into a patient the morning before they go into a surgery, or they can start on this therapy the very day they’re going to start a round of chemotherapy or radiation.
It bypasses first phase detox pathways of the liver, so it doesn’t interact, intervene, speed up or slow down detox processes that could otherwise cause some adverse events, or change the desired effect of a certain medication, herbal intervention or dietary intervention.”
Mistletoe Modulates Immune Function
Your immune system and metabolic function are both integral parts of addressing cancer, and mistletoe works on both. It’s important to recognize, however, that it’s not a magic bullet. If you’re eating a standard American diet and are metabolically dysfunctional, mistletoe is not going to be as effective as for someone who is also eating a healthy whole food diet and supporting their health in other ways.
That said, mistletoe is an immunomodulator. Immune therapies are all the rage right now, with a majority of research dollars being funneled into them. Yet the effectiveness rate for these therapies is less than 20%. In other words, they’re hardly a cure.
- 1 BitChute, Dr. Nathan Goodyear Discusses Benefits of Vitamin C in Cancer Treatment August 3, 2022
- 2 NIH National Cancer Institute, Cancer Statistics
- 3, 4, 5, 6, 9 STAT News August 15, 2023
- 7 Journal of Clinical Oncology 41, no. 17_suppl (June 10, 2023) LBA7505-LBA7505
- 8, 11 N Engl J Med 2022; 386:923-932
- 10, 13 STAT News March 9, 2022
- 12 N Engl J Med 2012; 366:1663-1673
- 14 NIH National Cancer Institute, Radiation Therapy Side Effects
- 15, 16 Radiat Oncol J. 2018 Jun; 36(2): 85–94. 3. Gynecological malignancies
- 17 American Cancer Society, Second Cancers Related to Treatment
- 18 BitChute, Dr. Mercola Interviews Susan Wadia-Ells May 6, 2021
- 19 BMJ 2023;382:e074520
- 20 Medical Xpress August 16, 2023
- 21 BMJ 2023;382:e074520, Comparison with other studies
How Curcumin Targets Cancer
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2023/07/25/curcumin-health-benefits.aspx
The original Mercola article may not remain on the original site, but I will endeavor to keep it on this site as long as I deem it to be appropriate.
Analysis by Dr. Joseph Mercola Fact Checked July 25, 2023
STORY AT-A-GLANCE
- The bioactive ingredient in turmeric is curcumin, responsible for over 150 potentially therapeutic activities in your body
- Curcumin has demonstrated preventive and treatment actions against cancer cells, and may help both reduce the negative effects of chemotherapy agents and intensify the cancer-killing abilities of the drugs
- Consumed alone, bioavailability of curcumin is poor; however, there are methods that may improve absorption and help raise your therapeutic levels
Editor’s Note: This article is a reprint. It was originally published September 17, 2018.
Turmeric, a yellow curry spice used in Indian cuisine, has a long history of medicinal use in traditional Chinese medicine (TCM) and Ayurvedic medicine. Curcumin is one of the most well-studied bioactive ingredients in turmeric,1 having over 150 potentially therapeutic activities, including anti-inflammatory, antimicrobial and powerful anticancer actions.
Cancer has an incredible global impact and places a vast financial and emotional burden on the families it touches. Nearly 40% of American men and women will be diagnosed with cancer in their lifetime and over $125 billion is spent annually on medical treatment and patient care.2
The American Cancer Society estimated there would be over 1.6 million new cases diagnosed in 2017, equating to 4,630 new cases and 1,650 deaths every day.3 The most common types of cancer include breast, colon, lung and prostate.4
Despite advances in cancer treatment protocols, scientists realize prevention plays an essential role in reducing the number of people who die from the disease. After 30 years of testing more than 1,000 different possible anticancer substances, the National Cancer Institute announced that curcumin has joined an elite group that will now be used in clinical trials for chemoprevention.5
Curcumin May Play a Multitargeted Role Against Cancer Cells
In this interview, Dr. William LaValley discusses the interaction curcumin has on cancer and the multiple ways this molecule affects cancer growth. If you have ever been diagnosed with cancer, it may feel as if it grew overnight when, in fact, cancer cells take years to develop.
The progression of a cell from normal growth to cancer happens through several stages. Deregulation of physiological and mechanical processes that initiate and promote the growth of cancer cells makes use of hundreds of genes and signaling routes, making it apparent a multitargeted approach is needed for prevention and treatment.
Research has demonstrated that curcumin has a broad range of actions as it is able to affect multiple cellular targets.6 Studies have found, based on the activities of curcumin in the body, the spice could be an effective method of cancer prevention, or in treatment when used in conjunction with conventional treatment protocols.
The multifaceted action of curcumin has made it useful in the treatments of several different types of diseases, including colon cancer,7 pancreatic cancer8 and amyloidosis.9
Curcumin triggers a variety of actions that affect the growth, replication and death of cancer cells. Cancer cells lose the ability to die naturally, which plays a significant role in the hyperproliferation of cells common to cancer. Curcumin is able to turn on the apoptosis (cell death) signaling pathway, enabling the cells to die within a natural time span.10
Cancer cells thrive in an inflammatory environment. Although short-term inflammation is beneficial for healing, long-term inflammation increases your risk of disease. Curcumin is able to block the pro-inflammatory response at several points and reduce the levels of inflammatory cytokines in the body.11
The strong anti-inflammatory effects of curcumin may match the effect of some drugs.12 Early in development, cancer cells learn to replicate and grow in an environment cells normally find inhospitable. Curcumin may change the signaling through several pathways, and put a stop to this replication.13
Curcumin may also stop the ability of cancer stem cells from replicating and reduce the potential for recurrence after treatment. Curcumin also helps support your immune system, capable of seeking out and destroying early cancer cells naturally.
Curcumin May Enhance Cancer Treatment and Chemotherapy
Some of the same ways that curcumin works in your body are the processes used to enhance your cancer treatments and chemotherapy.
While some chemotherapy has been developed to target specific cells, most therapy drugs are nonspecific and affect all cells in your body. Some studies in the past decade have demonstrated exciting potential for curcumin in the fight against cancer.
In addition to changes to your cells mentioned above, researchers have found curcumin may help protect your body against the damage caused from chemotherapy and radiation treatments, and it may enhance the effect of these same treatments, making them more effective.
These effects have been demonstrated in animal models treating head and neck tumors,14 and in culture of human breast, esophageal and colon cancers.15,16
Patients treated for chronic myeloid leukemia with chemotherapy exhibited a reduction in cancer growth factor when curcumin was added to the treatment protocol, potentially improving the results of the chemotherapy over being used alone.17
Protection against radiation therapy was demonstrated in a study using breast cancer patients receiving radiation therapy.18 At the end of the study those taking curcumin had less radiation damage to their skin.
Curcumin has also been effective against angiogenesis in tumors, or the growth of new blood vessels to feed the overgrowth of cancer cells, and against metastasis.19
Curcumin is able to affect cancer cells through multiple pathways and has fulfilled the traits for an ideal cancer prevention agent as it has low toxicity, is affordable and is easily accessible. However, while effective, it has poor bioavailability on its own.20
Download this Article Before it Disappears
Poor Absorption Has One Benefit
In my interview with LaValley, he discussed the poor bioavailability of curcumin in raw form. Only 1% of the product will be absorbed; even supplements that have a 95% concentration are absorbed at 1%.
This means, when the supplement is taken alone, it is a challenge to maintain a therapeutic level. However, in the case of colon cancer, this poor absorption into the bloodstream may be an advantage.
As there is poor absorption, higher levels of curcumin stay in the intestinal tract for longer periods of time, having an effect on gastrointestinal cancers. In one study, participants took a 1,080 milligram (mg) dose per day of curcumin for 10 to 30 days between their initial biopsy and surgical removal.
The patients taking the supplement experienced a reduction in blood levels of inflammatory agent, improvement in their body weight and an increased number of dying tumor cells.21
A team of scientists at the University of Pittsburgh and at Pondicherry University, India, discovered the bioactive ingredient in turmeric, curcumin, can both prevent and cure bowel cancers.22 The team found the compound triggered cancer cell death by increasing a level of protein labeled GADD45a.23 Lead author Rajasekaran Baskaran, Ph.D., who has more than 20 years of experience in cancer research, commented:24
“Studies on the effect of curcumin on cancer and normal cells will be useful for the ongoing preclinical and clinical investigations on this potential chemopreventive agent.”
As an increased bioavailability and absorption may also improve the actions of curcumin in the body, researchers have studied a variety of different delivery methods, including oral, intravenous, subcutaneous and intraperitoneal, as well as different formulations of the product.25
Bioavailability improved when curcumin was delivered as a nanoparticle, in combination with poly(lactic)-co-glycolic acid, liposomal encapsulation26 and when taken orally with piperine, the active ingredient in black pepper.27
Multiple Types of Cancer Affected by Curcumin
Research demonstrates that while curcumin has multiple pathways through which it impacts cancer cells, the substance also has an effect on multiple types of cancer. Studies estimate that genetics may play a role in approximately 5% of all cancers, with the majority of cancer growth attributed to lifestyle choices.28
Research demonstrates curcumin exhibits activity against breast cancer and decreases the toxic effect against some of the chemotherapy agents commonly used.29 Mitomycin C is a potent antineoplastic drug. However, prolonged use may lead to kidney and bone marrow damage, with secondary tumor growth. Curcumin appears to reduce the side effects of Mitomycin C and improve the efficiency of the drug at the same time.30
Another study demonstrated that curcumin inhibited the growth and metastasis of lung cancer cells.31 One of the deadliest cancers worldwide, pancreatic cancer, also appears to respond to the use of curcumin in preclinical trials.32 The antiproliferative effects on pancreatic cancer appeared to be from a reduction in oxidative stress and angiogenesis and triggering apoptosis of cancer cells.
Apoptosis, anti-inflammatory actions, reduction in angiogenesis and reduction in the adverse effects of chemotherapeutic agents has also led researchers to consider curcumin an adjunctive therapy in the treatment of liver cancer.33 Curcumin also inhibited and slowed the development of bladder cancer in rats,34 stopped the formation of metastasis in prostate cancer,35 and when combined with ultrasound, increased death of cervical cancer cells.36
But not all scientists are convinced by the number of studies over the past 15 years demonstrating the multiple effects curcumin has on the inflammatory response and cancers, as well as the low toxicity profile.37 In one meta-analysis, researchers claimed curcumin could not meet the criteria for a good drug candidate.38
More Benefits to Curcumin
Curcumin offers additional benefits to your health. It may work as well as some anti-inflammatory medications to treat arthritic conditions.39 In combination with aerobic exercise, curcumin was found to improve endothelial cell function in postmenopausal women,40 and was also found to ameliorate arterial dysfunction and oxidative stress in the elderly.41
Disease processes may increase oxidative stress and free radical formation in your body. Curcumin is a potent antioxidant,42 but also may boost the function of your body’s own antioxidant enzymes.43
Your brain can develop new connections powered by brain-derived neurotrophic factor (BDNF).44 Reduced levels of this hormone may be linked to depression and Alzheimer’s disease. However, curcumin can increase your levels of BDNF45 and effectively reduce your potential for suffering from age-related reduction in brain function.46
Researchers have also discovered that curcumin has an effect on several pathways in your body that may reverse insulin resistance, hyperlipidemia and other symptoms associated with metabolic syndrome and obesity.47 The reduced potential for metabolic syndrome and obesity is related to the anti-inflammatory effects of curcumin, which may also have an effect on heart disease, atherosclerosis and Type 2 diabetes.48
Genetic Regulation May Be One Way Curcumin Fights Cancer
It is becoming widely accepted that cancer is not a preprogrammed inevitability, but rather the result of the impact of your environment on genetic regulation that may trigger cancer cell growth. There are multiple influences that may damage or mutate DNA, and consequently alter genetic expression, including:
| Nutritional deficiencies | Stress |
| Free radical damage | Toxins and pollution |
| Chronic infections | Infectious toxic by-products |
| Hormonal imbalances | Chronic inflammation |
Researchers have demonstrated curcumin may affect more than 100 different pathways in your cells, helping to prevent hyperproliferation of cell growth characteristic of cancer, and aiding in the treatment of the disease. Through the reduction of inflammation, prevention of the development of additional blood supply to support cancer cell growth and destruction of mutated cells to reduce metastasis, curcumin has great medicinal and preventive potential.
Several studies have demonstrated an impact on transcription factors and signaling pathways, and have reviewed the molecular mechanisms curcumin uses to regulate and modulate gene expression.49,50,51 Overall, curcumin is powerful, cost-effective and has a low toxicity profile.52
Using a Curcumin Supplement
Turmeric is a wonderful spice used in Eastern culture cuisine. It is one spice I recommend for your kitchen as it works well with tomato sauces, soups, leafy greens, cauliflower, stir-fries and stews. Choose a high-quality turmeric powder instead of curry powder as studies have found some curry powders have very little curcumin.
If you are looking for therapeutic effects, you may want to consider a supplement. It is difficult to achieve a dose of curcumin used in research solely from your diet. Typical anticancer doses range between 8 grams and 12 grams of curcumin.
You can increase the absorption by making a microemulsion, combining 1 tablespoon of curcumin powder with one or two egg yolks and 1 to 2 teaspoons of melted coconut oil, as the curcumin is fat soluble. Then use a hand blender on high speed to emulsify the powder.
Absorption may also be increased through boiling. Add 1 tablespoon into a quart of boiling water. (If you add it to room temperature water and then boil, it doesn’t work as well.) After boiling it for 10 minutes, you will have created a 12% solution and you can drink this once it has cooled down. The curcumin will gradually fall out of the solution over time, and in about six hours it will be a 6% solution, so it is best to drink the water within four hours.
Curcumin is a very potent yellow pigment and can permanently discolor surfaces if you aren’t careful. To avoid inadvertently staining your kitchen yellow, I recommend you perform any mixing under the hood of your stove with the exhaust fan on to make sure no powder gets into your kitchen.
Alternatively, it is far easier to take curcumin in supplement form — just make sure it’s a high-quality brand that is formulated to increase bioavailability. And, look for a turmeric extract with at least 95% curcuminoids. Just be aware that these are relatively rare and hard to find.
- 1 Scientific American March 25, 2015
- 2, 4 National Cancer Institute, Cancer Statistics
- 3 American Cancer Society, Cancer Statistics Center
- 5 Cancer Prevention Research 2013; 6(5):387-400
- 6 Toxins 2010; 2(1):128-162
- 7 Current Pharmaceutical Design 2002; 8(19):165-1706
- 8 Integrative Cancer Therapies 2016; 15(3):333-334
- 9 Scientific Reports, 2016; 6(26623)
- 10 Current Cancer Drug Targets, 2005; 5(2):117-129
- 11 International Journal of Biochemistry and Cell Biology, 2009;41(1):40-59
- 12 Alternative Medicine Review 2009; 14(2): 141
- 13 LifeExtension, September 2016
- 14 Molecular Cancer Therapeutics 2010; 9(10) 2665
- 15 Translational Oncology 2010; 3(2):99-108
- 16 International Journal of Radiation Oncology 2009; 75(2): 534
- 17 Journal of Oncology Pharmacy Practice 2012;18(2):186
- 18 Radiation Research, 2013; 180(1):34-43
- 19, 52 American Association of Pharmaceutical Scientists Journal, 2009;11(3): 495
- 20 Cancer Prevention Research, 2013; 6(5): 387
- 21 Cancer Investigation 2011; 29(3):208
- 22, 24 Times of India, March 10, 2016
- 23 Molecular and Cellular Biochemistry, 2016; 414(1-2): 13-22
- 25, 26 Cancer Research Treatment 2014; 46(1): 2-18
- 27 Nutrition Facts, February 5, 2015
- 28 Cancer Letters, 2008; 267(1):133-64
- 29, 30 Journal of Breast Cancer 2013; 16(2) 133-137
- 31 Oncotarget 2016; 7(18):26535-26550
- 32 Nutrients 2016; 8(7):E433
- 33 Hepatoma Research September 3, 2016 Home Articles Article Topic: Natural Products and Hepatocellular Carcinoma
- 34 Cancer Letters 2008; 264(2): 299 – 308
- 35 Medical News Today, October 2012
- 36 European Journal of Obstetrics, Gynecology and Reproductive Biology 2015; 193:96-101
- 37 Forbes January 19, 2017
- 38 Journal of Medicinal Chemistry 2017;The Essential Medicinal Chemistry of Curcumin
- 39 Journal of Alternative and Complementary Medicine 2003; 9(1):161-168
- 40 Nutrition Research 2012; 32(10):795
- 41 Experimental Gerontology 2014; 48(2):269-276
- 42 Advances in Experimental Medicine and Biology 2007; 595:105-125
- 43 Toxicological and Environmental Chemistry 2013; 95(6)
- 44 Growth Factors 2004; 22(3):123-131
- 45 Brain Research 2006; 1122(1):56-64
- 46 PLOS|One February 2012
- 47 European Journal of Nutrition 2011; 50(3):151-161
- 48 Annual Review of Nutrition 2010; 30:173
- 49 Biofactors 2013; 39(1):37-55
- 50 Nutrition and Cancer 2012;64(4):607-616
- 51 Anticancer Research 2010;30(10):4007
The Plan to Tag Us for the New World Order Slave System
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2022/01/16/new-world-order-slave-system.aspx
The original Mercola article may not remain on the original site, but I will endeavor to keep it on this site as long as I deem it to be appropriate, and will not be bullied into removing it.
Analysis by Dr. Joseph Mercola Fact Checked January 16, 2022
STORY AT-A-GLANCE
- Dozens of peer-reviewed studies show that when COVID-19 is treated within the first few days of symptom onset, there’s an 85% reduction in hospitalization and death
- With Omicron, we have been gifted a best-case scenario. The highly contagious virus can rip through the population, causing only mild cold symptoms, thus producing herd immunity without the risk of mass casualties
- Two months before the rollout of the COVID shots, the U.S. Food and Drug Administration was aware that they could cause serious problems, including heart attacks, strokes, myocarditis, blood clots, neurological problems and more, yet they pushed them anyway
- Dr. Vladimir Zelenko believes SARS-CoV-2 is a bioweapon. Patents spanning two decades support this view. Those who created the weapon also investigated and identified antidotes, which includes the zinc ionophore hydroxychloroquine
- The antidote to COVID was intentionally suppressed to encourage people to get the COVID jab, which Zelenko believes is a tool to tag people for the New World Order slave system
Dr. Vladimir Zelenko, whom I’ve interviewed twice previously, was among the first U.S. physicians to develop an early treatment program for the novel SARS-CoV-2 infection. He popularized the use of hydroxychloroquine and zinc, and when hydroxychloroquine became increasingly difficult to obtain, he was also among the first to identify quercetin as a viable alternative.
When the pandemic started, Zelenko was practicing in New York. He has since moved to Florida, where he’s been giving interviews for several hours a day, trying to spread the word about early treatment and prevention. As noted by Zelenko:
“It’s a very treatable infection — or should I say bioweapon? — if done within the first few days, because COVID is two diseases. It’s the infectious stage of the virus, and then a week later, you have the pathogenic inflammatory reaction that does all the damage to the lungs and causes blood clots.
So, it’s all about timing. And the data is very clear. There are dozens of peer-reviewed studies that prove if you treat COVID within the first few days, you have an 85% reduction in hospitalization and death. It’s a no-brainer. You could have saved 700,000 people from going to the hospital out of 800,000.”
While licensed to practice medicine in Florida, Zelenko now spends most of his time educating the public and other doctors. He’s also available via telemedicine, but his passion has become researching and developing simple, natural approaches to complex health problems — including his own.
The Road Less Traveled
Zelenko has a rare type of cancer called pulmonary artery sarcoma, which is typically fatal. He’s also undergone two open-heart surgeries and three years of chemo and radiation, none of which has resolved his problems.
“Almost four years ago, I was diagnosed with pulmonary artery sarcoma. There are only 10 cases on average per year, and they’re all found at autopsy. In my case, they thought it was a blood clot that didn’t respond to blood-thinning medication.
So, the decision was made to do an embolectomy, open my chest, go into the pulmonary artery and take out the blood clot. But when they did that, they saw it was a tumor, and it had completely destroyed my right lung. So, I lost my right lung. And they resected a large part of the pulmonary artery and had to reconstruct it because you need that artery to live.
Then I was in chemo … I was pretty good for two years, and then it came back and had spread to my hip as well. And so, I had another open-heart surgery. They had to replace one of my heart valves, pulmonic valve. Then I went for radiation to my hip [followed by] really heavy chemo.
After two months on that, I went into congestive heart failure and developed cardiomyopathy … I recovered from that, and was put on heart failure medication … A month after that … I developed COVID pneumonia … I was pretty sure I was going to leave in a box, yet I recovered.
A few months later, I went for another CT scan, and they found, again, the tumor was back in the pulmonary artery, but this time, no doctor wanted to operate on me. A third open-heart procedure is very dangerous. They estimated more than 50% likelihood I would die on the table, which I didn’t like. So, I ended up having pretty intense radiation to my mediastinum, where the tumor was.
That’s when you came into the picture, in terms of advising me about treatment. I ended up having immunotherapy in Europe for two months with checkpoint inhibitors, but also hyperthermia and mistletoe injections, and alpha lipoic acid, high-dose vitamin C [infusions] and different other modalities. And I feel better than ever.
I had a CT scan last week, and it showed the tumor shrank by one-third. I spoke to the radiation oncologist who told me that a good result would’ve been the same size or smaller. It takes years to resolve. So, time will tell, but it’s easier for me to walk, and hemodynamically I’m more stable, and I feel good. Amen.”
The Surprising Role of Immunotherapy in Cancer
Overall, the “COVID story has completely changed the way I look at life,” Zelenko says. When he saw how natural, effective, over-the-counter solutions for COVID were suppressed, while experimental gene transfer shots were pushed, he realized other treatments might also be suppressed, such as cancer treatments.
“Probably, effective approaches were marginalized in lieu of the more expensive pharmaceutical approaches,” he says. “I’ll give you one example. Dr. [William] Coley was an oncological surgeon who lived around 100 years ago, maybe 120 years ago. He noticed that he would operate on his patients, and the tumor would come back and they would die. And then he observed something very interesting.
He had a patient with pancreatic cancer, Stage 4, inoperable. That patient got very sick with an infection and became septic. He almost died, but he recovered and his tumor went away. He noticed that type of phenomenon a few more times, and realized that there must be some immune reaction, immune response to the infection that wakes up the immune system to also attack the tumor.
So basically, in my opinion, that was the birth of immunotherapy. Fever seems to play a role. It seems to have antitumor properties, as well as activating certain parts of your immune system. So, it’s fascinating. And that information was buried for a good long time — 50, 60 years — until some doctors rediscovered it and started doing research. And I benefited from that in Europe.”
Hyperthermic Treatment for Cancer
We’ve come a long way since the days of Coley, who used toxins to trigger infection and fever. Today, hyperthermic treatment is used instead. Basically, it’s all about raising your body temperature to about 104 degrees Fahrenheit for four to six hours. Zelenko describes the treatment he underwent:
“It was quite an experience, having a temperature around 40 Celsius, let’s say 104 degrees Fahrenheit, for five hours. You become a little loopy and a little anxious, but I drank a lot of fluids and had a nurse with me all the time. It was a pretty interesting experience.
There were whole-body hyperthermia machines and localized hyperthermia. Both are basically a fancy sauna. It was like a spa actually. I did enjoy the treatment in most cases.”
As an aside, I sincerely believe sauna bathing is one of the most powerful biohacks available. I do it four times a week. I get my temperature up to about 102 degrees F. or so, for 20 minutes. I’ve found it to be a profoundly effective health habit to nip infections in the bud, and may also help put the brakes on any potential malignancies. I am currently using a prototype full-spectrum SaunaSpace sauna that is EMF-free, has eight 250 watt bulbs and will likely be available later this year.
Omicron Is Unstoppable, But Not To Be Feared
Getting back to the issue of COVID, over the past two years, the SARS-CoV-2 infection has gone through a number of changes. Omicron, for example, is far more contagious, but has far less severe symptoms. As noted by Zelenko:
“Omicron is unstoppable. It’s more infectious than measles. Everyone’s going to get it. Sorry, but that’s the case. However, it seems to attack only the upper airway in most cases, and there are very few deaths. It’s very responsive to treatment as well, so there’s no reason to be afraid of it.”
In fact, we appear to have been gifted a best-case scenario, in which a highly contagious virus will rip through the population, causing only mild cold symptoms, thus producing herd immunity without the risk of mass casualties. “When two-thirds of the population gets through it, it essentially shuts down the pandemic,” Zelenko says.
Vaccinating During a Pandemic Breeds Variants
In the interview, Zelenko explains how the many variants we’ve seen have probably been a result of the mass “vaccination” campaign.
Three respected immunologists, Dr. Luc Montagnier (who won the Nobel Prize in 2008 for his discovery of the HIV virus), Dr. Sucharit Bhakdi, the most published immunologist in history, and Dr. Geert Vanden Bossche, a top immunologist in The Netherlands, have all warned that when you mass vaccinate in the middle of an active outbreak, you cause variants to emerge.
“You exert evolutionary pressure and breed more varying viruses,” Zelenko says. “Now, there are two or three possibilities. One could be that it was unintentional. Good, well-meaning people developed what they thought would help — a vaccine. However, giving it to people during a pandemic has been an absolute failure. ‘Oops, we’re sorry.’ That’s one possibility.
The other possibility is that whoever has orchestrated this knows exactly what they’re doing, and they are doing it on purpose to maintain the new variants and the consequences of that, which is essentially a psyop [to cause] a global psychosis due to fear, lockdowns and wearing a face diaper.
There’s one more possibility. There’s no dispute; everyone who knows the facts and has studied the issue knows that COVID-19 is a weapon made in a laboratory. Gain-of-function research is nothing more than making a weapon of mass destruction and genocide, and there’s a patent trail 20 years long that documents the different stages of development of this weapon.
And here’s my supposition. I have no evidence of this, but I could say the following: If I could make the original virus, I could make variants. It’s very easy. You just change a few sequences of the code that goes with the spike protein. You change its three-dimensional shape, and if you do it enough, eliminate existing antibodies.
So again, I don’t have evidence for that, but I do have evidence that [SARS-CoV-2] is an artificially-made bioweapon. So why wouldn’t it be possible to make variants the same way? I think it’s kind of a combination, multifactorial cause of variants — the natural God factor, the evolutionary pressure exerted by vaccinating people during an active pandemic, and then just outright making them.”
Antidotes to the Bioweapon Were Developed Beforehand
Zelenko goes on to recount a relatively recent realization. Back in March 2020, he saw a MedCram video, episode 34,1 in which Dr. Roger Seheult explained some of the principles that he then ended up building his COVID protocol on. Seheult specifically quoted a paper that explained the functioning of zinc ionophores.
That mechanism is what Zelenko relied upon when developing his own protocol. However, he didn’t realize until December 2021 that the author of that central paper was Dr. Ralph Baric. Why does that matter? Zelenko explains:
“In 1999, Ralph Baric, funded by the U.S. government, at the University of North Carolina at Chapel Hill, figured out how to take an animal virus and have it be able to infect other species, different animals, in other words, cross-species infection.
In 2015, the same Dr. Ralph Baric, and Dr. Zhengli [at the Wuhan Institute of Virology in China], funded by the National Institutes of Health, figured out how to make a corona bat virus infect human beings, and augmented its lethality to human lives. That was in 2015. But in 2010, Baric published that paper that I’m referring to.
So, the development of the weapon happened in stages, but before it was unleashed onto the human population, or the development of it being able to infect human beings, an antidote was made. Research paid for by the government was published.
The same people that made the bomb, let’s say, also created the antidote to diffuse the bomb. And then, when the pandemic arrived, doctors like myself, out of necessity, came up with creative solutions, based — in my case, unknowingly — on this work. And immediately, that information was marginalized and suppressed, and doctors were deplatformed for advocating for it.
So, the government who made the bomb also knew about the solution. And the reason why is they didn’t want to die. The stakeholders here don’t want their families to die. But for you and for me, they have a different agenda. So, they had that information.
I have knowledge that the Google executives are all taking hydroxychloroquine and ivermectin for prophylaxis, as is half of Congress. And so, the people that have orchestrated this knew the answer, and use it for themselves. Even doctors know the answer for themselves.
They prescribe [these drugs] for themselves, or they call me. But when patients come, they say there’s no treatment, go home, take Tylenol. So, this is mass murder.”
The COVID Jabs — Another Crime Against Humanity
In addition to killing untold numbers of people by denying and suppressing early treatment options, governments around the world are also killing people with the COVID jabs. A year into the aggressive campaign to inject as many people as possible, it’s likely the shots have killed more people than have died from the infection. It’s very difficult to tell, unfortunately, because the data are so seriously manipulated.
Zelenko estimates somewhere between 500,000 to 1 million Americans have been killed by the shots to date. Disturbingly, the U.S. Food and Drug Administration was aware that the shots could have serious consequences, yet they pushed them anyway. What’s more, they refuse to address the mindboggling number of adverse events reported to the Vaccine Adverse Events Reporting System (VAERS). The safety signal couldn’t possibly be clearer.
“In October, 2020, two months before the vaccine rollout, there was an internal presentation in the FDA to its scientists, and on slide 16 of that presentation, there was a list of side effects: death, heart attack, stroke, blood clots, horrific neurological diseases, myocarditis and many, many more,” Zelenko says.
“Now keep in mind, this is two months prior to the rollout. After the vaccines were rolled out, and a few months into it, when the VAERS database started showing the side effects that people were experiencing, there’s a 100% correlation with what that slide said would happen, and what actually happened to human beings.
That is premeditated mass murder. FDA knew exactly what it was doing. They knew exactly the side effects, and they released it anyway …”
What’s the Real Agenda?
Why would the FDA behave this way? Why aren’t they safeguarding public health from a clearly lethal treatment? And on the other hand, why aren’t they allowing doctors to help people with early treatment? Zelenko explains:
“In the mid-‘90s, it became obvious that the American economy was doomed. The Medicare and Social Security systems would become insolvent, and that would cause a tsunami-like effect nationally and internationally. And it was unstoppable. It was [mathematically inevitable].
Medicare, according to Congressional Budget Office, in 2027 will begin the process towards bankruptcy. So, security as of today [will last until] 2034. Now, the major stakeholders in the world economies saw an existential threat. They understood that their power and wealth was in real jeopardy.
And so a plan was developed, which was beyond the technology at that time, but the technology was being developed. So, for example, the Human Genome Project was mapped and completed.
Then CRISPR technology was developed, which is gene editing or gene splicing in very precise ways. That was sold as a way to cure genetic diseases. There’s a defective gene. You can just cut it out and splice in, cut and paste, basically, a healthy gene.
That’s the upside. The downside is that it creates possibilities to do gene editing for nefarious reasons. In 2015, Bill Gates said that the world population needs to be reduced by 15% through the use of vaccines because of global warming.
The same Bill Gates in 2020 said 7 billion people must be vaccinated. So, the obvious rhetorical question is, ‘Why would I take a vaccine for my health from someone who’s advocating the use of vaccines to reduce the world population?’
In 2016, Klaus Schwab, in an interview said something very strange. He said that within 10 years, by 2026, every single human being will be tagged with a digital identifier. What does that mean, and why?
Let’s go through the sequence of events. A bioweapon is made with an antidote, which is being suppressed and hidden. [The bioweapon] is released. It’s extremely easy to treat. However, that information is being suppressed, and access to those medications is being suppressed, and doctors who are advocating for it are being persecuted.
Anything that seems to give people hope, lessen anxiety, encourage reintegration with your loved ones seems to be immediately vilified, even early intervention. If you look at the NIH, they recommend, as of today, not to treat COVID unless they’re in the hospital with lung damage. Don’t do that.
And so, I was wondering, what is really going on? And why this incessant push to vaccinate everyone? Why jail doctors for using meds at work? Because it encourages the vaccine hesitancy.
Then I realized something. There were two patents that I became aware of. They’re separated by a year, but they’re linked in the puzzle, in the concept. One was August 31, 2021, that describes … nanotechnology engineering.2 It basically describes the following:
That there is the capability, the technology, already existing, in these vaccines that allows for the measurement of biometric data, meaning your heart rate, your respiratory rate, temperature, and then the transmission of that data with your location to a third party.
That didn’t even make sense to me. Like what? But then I realized there’s another patent owned by Microsoft. This one I remember by heart. It’s an international patent, WO202060606. You can’t make this stuff up. That patent describes linkage of biometric data transmission to cryptocurrency.
Then I got it. And by the way, 2026, when everyone’s supposed to be tagged with a digital ID, let’s call it an internal Auschwitz tattoo, is a year before the beginning of the insolvency of Medicare and the beginning of economic collapse. And so, the real agenda has become obvious to me.
It’s never been about health. COVID-19 is easy to treat. It was always about using fear and mass psychosis to get 7 billion people to willfully get injected with the technology that would permit them to participate in the new cryptocurrency-based system, the system that the world will use for finance.
Fiat currency and all the traditional ways of transactions will be gone. The only way that you actually will be able to participate in transactions, of buying bread, let’s say, is having a transmitting sensor of information with your location. It’s the mark of the beast, if you really want to know. With that, you can then buy bread for your family …
Gates and Schwab [are] both talking talk about how these vaccines change who you are. What does that mean? They explain it. [With] the gene editing technology, they are making the human better. That’s transhumanism. I call it Human 2.0. Human 1.0 is the version made by God. We are is imprinted [with God] in our genetic code. We’re made in the image of God because we have his code in us.
Now, would you give Bill Gates or Klaus Schwab the password to your home security system? Why would we give him access to our genetic code? Human 2.0, in the demented, depraved, deranged minds of these people is the next step up in the evolution of human beings. And I’m saying that if you allow that to happen to yourself, you’re no longer made in the image of God. You’re made in the image of Bill Gates and Klaus Schwab.”
A Ploy to Tag Us for the NWO’s Slave System
So, in summary, Zelenko believes that everything we’ve experienced so far — the aggressive marketing of the shots, the coercion and threats made to get as many injected as possible — has all been a ploy to “tag” as many people as possible in preparation for the New World Order’s cryptocurrency system, which will be managed by a small select group, and used to enslave all of humanity.
As noted by Zelenko, the World Economic Forum has publicly announced that by 2030, the U.S. will no longer be a superpower, and a few countries will be in charge of global governance. Now, how do you destabilize an economic engine like the U.S.?
“You create a pandemic,” Zelenko says. “You lock down middle class businesses, small businesses … But you leave Walmart and Home Depot open … It’s a wealth transfer from the middle class to the people in power. It’s a robbery, basically.
This is one big attempt at enslaving humanity. It’s a brilliant plan, by the way. It’s evil, but it’s brilliant because slavery has always been the most lucrative industry and asset throughout human history. Now is no different. And so, you have a few sociopaths who believe in their immortality and think that they’ll transfer their consciousness to some cyborg, enjoying the whole world as their playground.”
Zelenko goes on to discuss the statements inscribed on the Georgia Guidestones, a huge granite monument erected anonymously in a small town in Georgia, which lays out 10 commandments. The first one is that the world population should be reduced to and maintained at 500 million. If the COVID shots continue, it’s not inconceivable that the human population might be reduced to that size.
The Why Behind the Genocide
A few months ago, Elon Musk debuted his humanoid robots, saying that since these robots will eliminate 90% of the workforce, we therefore need universal basic income. This too is part of The Great Reset plan, which embraces both technocracy and transhumanism.
“Keep in mind that in the minds of these people, we’re not made in the divine [image]. We’re cockroaches. And they’re not going to throw endless universal income resources at cockroaches for too long. They’ll do it initially to identify the useless eaters, and then they will be liquidated. This has happened before.
Just 80 years ago you had the Nazi ideology based on eugenics, which created three classes of people. You have the ubermensch, what Nietzsche would call Superman. Then the mensch, which is the human, and then the untermensch, which is the subhuman. In the [Nazi] model, the [Nazis were] Supermen, descendants of Aryan gods. That gave them the power to enslave others.
So, for example, the Anglo-Saxons, basically Europeans, were meant to be slaves to the Aryans. And the subhumans, which I belong to — Jews, gypsies, Slavs, handicapped, political prisoners — we were meant to be vaporized, become dust.
That ideology did not go away. It resurfaced with the nuance that is not antisemitic right now. In a kind of an abstract way, we’re all Jews this time, because the hierarchy here is not based on religion or identity, but rather on the deranged belief that they’ve evolved, the Superman of this generation, into a higher level of consciousness.
They’re woke and they understand and are enlightened about the nature of the human condition. They’re custodians of the planet, and therefore it’s their responsibility to make sure the planet has solvency, that it continues to exist. And therefore, we have to reduce the world population.”
Cause for Optimism
While humanity is in a most precarious situation, Zelenko is optimistic about the future.
“I’ll tell you what I really think is going on,” he says. “There’s what we see, and then there’s the, let’s call it spiritual physics, at play. Karl Jung, the famous psychoanalyst, wrote, ‘The moral degradation of society begins with the degradation of the individual.’ From that, we can actually learn that moral improvement of society begins with improvement of the individual.
We, as a society, over the last 50, 60 years, have made some very bad choices. For example, we’ve desanctified or defiled gender roles … Marriage has lost its sanctity. The unborn are being massacred. In the Bible, there are two cities that were destroyed, Sodom and Gomorrah, and there’s an analysis why that happened. It wasn’t because of the immorality, because the whole world was immoral.
It was because they codified immorality into the law of the land. That’s exactly what has happened in [the U.S.] We’ve devolved … We worship the God of science, the god of technology, the god of money, god of power. Anything but [the true] God. And we are clearly practicing child sacrifice.
Dr. Michael Yeadon, former VP of Pfizer, told me personally, and then he actually publicized it, that for every one child that dies of COVID, 100 die from the vaccine. The [COVID shot] is 100 times more lethal to children than COVID. What do you call that? That’s child sacrifice.
So, I feel that, by way of analogy, we’re in the generation of flood. The house is going to get cleaned, and each individual is given a choice to get on the ark or not.
Or, to make it simpler, who do you bow down to? Do you bow down to your creator, who makes you in every instant of time? Do you ask [God] for fortitude, endurance, strength, resolve, the ability to deal with the unknown and fear? Or are you going to give in to the fear and bow down to corrupt sociopaths, oligarchs, corrupt governments, and the false promise of the golden calf of these vaccines?
Because at this point, in this country at least, no one’s holding you down and putting a needle into your arm. The majority of people, they want to travel by plane. They don’t want to lose their job. They want to go to school. It’s all these kinds of quality of life decisions. In other words, in a normal society, the parents sacrifice for the well-being of the children. In pagan societies, we sacrifice the children for the purpose of the adults.”
Peaceful Civil Disobedience Is the Answer
So, what’s the answer? Can we stop this transhumanist trajectory that threatens the very core of what makes us human? Can we prevent this plan for our enslavement from coming to fruition? Zelenko believes there is a way, as do I.
“The answer is we need organized civil disobedience. Do not comply. They can’t imprison everyone. They can’t fire everyone. They can’t expel everyone. They can’t lock down everyone. There’s many more of us than them. And actually, let me speak to the military leaders, to the police, to people that are charged to protect society.
You also have children. You also have parents. And we are relying on you to do what’s best for the citizens of this country, to protect us from all enemies, foreign and domestic. All we need to do is to coalesce with like-minded people. Take your kids out of school. Homeschool them. You can teach them morality.
The World Health Organization came out with an edict that if your kids go to school, that’s implied consent for the vaccine because you could have not sent them. And since you sent them to school, that’s implying that you’re consenting for them to be vaccinated, even without your knowledge.
Basically, we have to make small pockets, like cities of refuge, in a sense, of like-minded people; create an alternate society; do commerce with ourselves. I know there are forces really working hard to create an alternate cryptocurrency or blockchain system that is decentralized and would allow for people who don’t want to be tagged with a digital identifier to transact with each other.”
As noted by Zelenko, it’s becoming more and more obvious that the pandemic measures were never about protecting us from COVID. It was always about creating a new world order. It was about setting the stage for a Great Reset to “Build Back Better.”
But better for whom? The Build Back Better plan is about building “a society run by a few sociopaths and the rest of us enslaved,” Zelenko says. The good news is that more and more people are now starting to see this plan, and “once that realization reaches a certain threshold of people, countries are going to change and fall like dominoes,” he says.
As for when we might get our freedom back, that depends on us. As noted by Zelenko, “freedom isn’t free.” We were free (at least up until 2020) because our forefathers had the courage to confront tyranny. If we want our children to be free, we now have to display that same courage.
“Whether or not our children will be free depends on whether or not we are ready to sacrifice,” Zelenko says. “Are we ready, in this generation, to pay the price to ensure that our children thrive in freedom and have the ability to maintain God consciousness?
It’s going to happen. The unknown variable is to body count. I would hope that this interview reaches the consciousness of every single human being. People must choose to say no from this point on.”
Dr. Peter McCullough: The State of COVID Treatment
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2021/09/18/the-state-of-covid-treatment.aspx
Analysis by Dr. Joseph Mercola Fact Checked September 18, 2021
STORY AT-A-GLANCE
- Cardiologist, internist and epidemiologist Dr. Peter McCullough discusses why a key aspect of care — early treatment — has been missing from the pandemic
- With no hope of early treatment, McCullough believes that most people became conditioned to wait for an injection
- COVID-19 injections are waning in effectiveness and linked to an unacceptable number of serious injuries and deaths
- McCullough is among a growing number of experts who believe COVID-19 injections are making the pandemic worse; indiscriminate vaccination is driving mutations, as the virus is mutating wildly to evade the injections
- At 53:40 in the video, you can view McCullough’s early treatment regimen, which initially includes a nutraceutical bundle, progressing to monoclonal antibody therapy, anti-infectives like HCQ or ivermectin, antibiotics, steroids and blood thinners
The video above,1 featuring cardiologist, internist and epidemiologist Dr. Peter McCullough, is packed with sound logic, data and action steps that have the potential to turn the pandemic around — if only more people would listen.
Recorded at the Andrews University Village Church in Berrien Springs, Michigan, August 20, 2021, this presentation deserves to be heard, and I urge you to listen to it in its entirety. It will make you question why a key aspect of care — early treatment — has been missing from the pandemic.
McCullough, editor of two medical journals who has published 650 peer-reviewed papers, said this has been the first time in his career when he saw medical providers not offering early treatment for a disease.
Early COVID Treatment Saves Lives
The standard of care for COVID-19 has been to withhold treatment until a person is sick enough to be hospitalized. It typically takes two to three weeks for someone with COVID-19 to get sick enough to be hospitalized, and during that time early treatment can be lifesaving.
The rationale was that there have been no large, randomized trials conducted to know which treatments are safe and effective, but as McCullough said, “We can’t wait for large randomized trials … Something got in the minds of doctors and nurses and everyone to not treat COVID-19. I couldn’t stand it.” He and colleagues worked feverishly to figure out a treatment — why didn’t national health organizations do so also?
“Our government and other governments, and the entire world, has not lifted a finger to reduce the risk of hospitalization and death anywhere,” McCullough said, pointing out the irony: “If there was a kid with asthma, would we let the kid wheeze and choke for two weeks before the kid has to go to the hospital? No, we give the child medications. We don’t have randomized trials for every single thing that we do.”2
McCullough and colleagues realized that there are three major phases to COVID-19. It starts with virus replication, which then triggers inflammation, or a cytokine storm. This, in turn, leads to blood clotting. If enough micro blood clots form in the lungs, a person can’t get enough oxygen and dies. It’s a complex process, and no single drug is going to work to treat it, which is why McCullough uses a combination of drugs, as is done to treat HIV, staph and other infections.
Only about 6% of doctors’ decisions in cardiology are based on randomized trials. “Medicine is an art and a science, it takes judgment. What was happening is, I think out of global fear, no judgement was happening,” McCullough said,3 referring to doctors’ refusal to treat COVID-19 patients early on in the disease process.
Doctors Threatened for Treating COVID-19
Around the world, the unthinkable is happening: Doctors are being threatened with loss of their license or even prison for trying to help their patients. French doctor Didier Raoult suggested, early on, putting up a tent to try to treat covid-19 patients. He was put on house arrest. He has promoted the use of hydroxychloroquine (HCQ), which initially was available over the counter — until France made it prescription only.4
In Australia, if a doctor attempts to treat a COVID-19 patient with HCQ, they could be put in prison. “Since when does a doctor get put in prison to try to help a patient with a simple generic drug?” McCullough said. In South Africa, he added, a doctor was put in prison for prescribing ivermectin.
In August 2020, McCullough’s landmark paper “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 Infection” was published online in the American Journal of Medicine.5
The follow-up paper is titled “Multifaceted Highly Targeted Sequential Multidrug Treatment of Early Ambulatory High-Risk SARS-CoV-2 Infection (COVID-19)” and was published in Reviews in Cardiovascular Medicine in December 2020.6 It became the basis for the home treatment guide.
While some physician organizations have stepped up and are treating COVID-19 patients, “The ivory tower today still is not treating patients. The party line in my health system is, do not treat a COVID-19 patient as an outpatient. Wait for them to get sick enough to be admitted. Because my health system … follows the National Institutes of Health or the Centers for Disease Control, period.”
Conditioned to Wait for an Injection
With no hope of early treatment, McCullough believes that most people became conditioned to wait for an injection. “We became conditioned, after about May or so, to wear a mask, wait in isolation and be saved by the vaccine. And wait for the vaccine. And all we could hear about is the vaccine.”
The injections were developed, but they’re different than any prior vaccines and have been losing effectiveness while causing an unacceptable number of serious injuries and deaths. For comparison, in 1976, a fast-tracked injection program against swine flu was halted after an estimated 25 to 32 deaths.7
According to McCullough in the video, if a new drug comes on the market and five deaths occur, the standard is to issue a black box warning stating the medication may cause death. With 50 deaths, the product is pulled from the market, he says. Now consider this: The Vaccine Adverse Event Reporting System (VAERS) database showed that — for all vaccines combined before 2020 — there were about 158 total deaths reported per year.
By January 22, 2021, there were already 182 deaths reported for COVID-19 injections, with just 27.1 million people vaccinated. This was more than enough to reach the mortality signal of concern to stop the program, McCullough said.
“We’ve already crossed the line of concern January 22. And if there was a data safety monitoring board — I know, because I do this work — we would have had an emergency meeting and said, wait a minute, people are dying after the vaccine. We’ve got to figure out why.”8
It’s standard to have an external critical event committee, an external data safety monitoring board and a human ethics committee for large clinical trials — such as the mass COVID-19 injection program, but these were not put into place.
“This is something we’ve never seen in human medicine — a new product introduced and just going full-steam ahead with no check on why people are dying after the vaccine,” McCullough said. On two occasions, the CDC and FDA — in March and in June — reviewed the data and said none of the deaths are related to the vaccines. “I think this is malfeasance,” he stated.
Fast-forward to July 30, 2021, and VAERS data showed 12,366 Americans have died after a COVID0-19 injection.9 In an analysis of COVID-19 vaccine death reports from VAERS, researchers found that 86% of the time, nothing else could have caused the death, and it appears the vaccine was the cause.10
The Spike Protein Is Dangerous
Your body recognizes the spike protein in COVID-19 jabs as foreign, so it begins to manufacture antibodies to protect you against COVID-19, or so the theory goes. But there’s a problem. The spike protein itself is dangerous and known to circulate in your body at least for weeks and more likely months11 — perhaps much longer — after the COVID jab.
In your cells, the spike protein damages blood vessels and can lead to the development of blood clots.12 It can go into your brain, adrenal glands, ovaries, heart, skeletal muscles and nerves, causing inflammation, scarring and damage in organs over time. McCullough also believes that the spike protein is present in donated blood, and they’ve notified the Red Cross and the American Association of Blood Banking.
Messenger RNA (mRNA) platforms have been under study for years, in most cases being designed to replace a defective gene, which could potentially be used for cancer or heart failure treatment, for example.
In November 2020, however, Pfizer, in a joint venture with Germany-based BioNTech, announced that their mRNA-based injection was “more than 90% effective” in a Phase 3 trial.13 This does not mean that 90% of people who get injected will be protected from COVID-19, as it’s based on relative risk reduction (RRR).
The absolute risk reduction (ARR) for the jab is less than 1%. “Although the RRR considers only participants who could benefit from the jab, the absolute risk reduction (ARR), which is the difference between attack rates with and without a jab, considers the whole population. ARRs tend to be ignored because they give a much less impressive effect size than RRRs,” researchers wrote in The Lancet Microbe in April 2021.14
McCullough believes the mass injection campaign is an incredible violation of human ethics, in part because no one should be pressured, coerced or threatened into using an investigational product.
No attempts have been made to present or mitigate risks to the public, such as giving it only to people who really need it — not to low risk groups like children and young people and those who are naturally immune to COVID-19 due to prior infection. “I think this is the most disturbing thing,” he said.
The Injections Don’t Stop COVID-19, Can Be Deadly
The CDC’s Morbidity and Mortality Weekly Report (MMWR) posted online July 30, 2021, details an outbreak of COVID-19 that occurred in Barnstable County, Massachusetts — 74% of the cases occurred in fully vaccinated people.15
Indiscriminate vaccination is driving mutations, as the virus is mutating wildly to evade the injections. Their effectiveness, too, is rapidly waning. A study published in medRxiv, using data from the Mayo Clinic Health System, revealed that during periods of Alpha and Delta variant prevalence, Moderna’s injection was 76% effective while Pfizer’s effectiveness was only 42%.16
A little-known fact is that Moderna’s jab has three times the dose of Pfizer’s, but, curiously, health officials aren’t even discussing this or giving the public updates on which of the three injections work “best.” The narrative is simple and straightforward — get an injection, any injection.
Yet, as McCullough noted, the virus has mutated, and the vaccines aren’t working the way health officials had hoped: “The vaccines don’t stop COVID-19, at least not completely, and they’re not a shield against mortality.”17
Similar to VAERS, the U.K. maintains a “Yellow Card” reporting site to report adverse effects to vaccines and medications.18
Tess Lawrie, whose company The Evidence-Based Medicine Consultancy has worked with the World Health Organization, analyzed U.K. Yellow Card data and concluded that there’s more than enough evidence to pull the injections from the market because they’re not safe for human use. The report stated:19
“It is now apparent that these products in the blood stream are toxic to humans. An immediate halt to the vaccination programme is required whilst a full and independent safety analysis is undertaken to investigate the full extent of the harms, which the UK Yellow Card data suggest include thromboembolism, multisystem inflammatory disease, immune suppression, autoimmunity and anaphylaxis, as well as Antibody Dependent Enhancement (ADE).”
Early Treatment Is Crucial
McCullough is trying to get the word out about the importance of early treatment of COVID-19. Early ambulatory therapy with a sequenced-multidrug regimen is supported by available sources of evidence and has a positive benefit-to-risk profile to reduce the risk of hospitalization and death.
At 53:40 in the video, you can view McCullough’s early treatment regimen, which initially includes a nutraceutical bundle. While you’re recovering at home, open your windows and get plenty of fresh air and ventilation in your home.
If symptoms persist or worsen, he recommends calling your doctor and demanding monoclonal antibody therapy. The treatment progresses to include anti-infectives like HCQ or ivermectin, antibiotics, steroids and blood thinners.
If your doctor refuses to treat COVID-19 in the early stages, find a new one and/or visit a telemedicine clinic that will help, as “the prehospital phase is the time of therapeutic opportunity.”
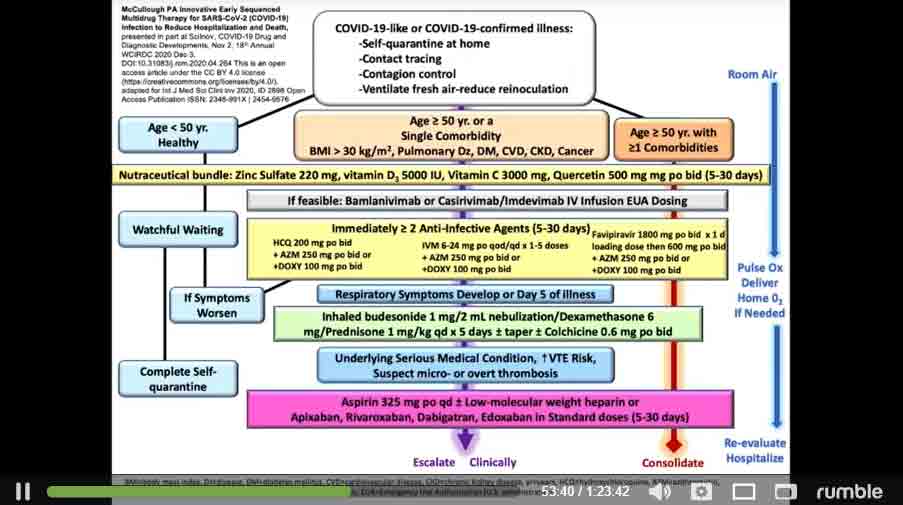
McCullough is among a growing number of experts who believe COVID-19 injections are making the pandemic worse. They “have an unfavorable safety profile and are not clinically effective, thus they cannot be generally supported in clinical practice at this time.”
Logically, this is clear, but McCullough believes we’re dealing with a mass psychosis that is preventing people from seeing the light. “The whole world is in a trance,” he said, adding:20
“Things are getting disturbingly out of control and it’s in the context of the virus. It is clear … we are in a very special time in the history of mankind. Whatever is going on, it is the entire world … every human being in the world. It appears to have a program.
The program … is happening to promote as much fear, isolation, suffering, hospitalization and death in order to get a needle in every arm, at all costs. That is what’s going on, and no one in this room can disagree.”
- 1, 2, 3, 4, 8, 9, 17, 20 Rumble August 26, 2021
- 5 American Journal of Medicine January 2021; 134(1): 16-22
- 6 Reviews in Cardiovascular Medicine 2020; 21(4): 517-530
- 7 CNN April 30, 2009
- 10 ResearchGate Preprint June 2021
- 11 Clinical Infectious Diseases, ciab465, doi: 10.1093/cid/ciab465
- 12 Bitchute July 22, 2021
- 13 Pfizer November 9, 2020
- 14 The Lancet Microbe April 20, 2021
- 15 MMWR Weekly August 6, 2021 / 70(31);1059-1062
- 16 medRxiv. 2021 Aug 9;2021.08.06.21261707. doi: 10.1101/2021.08.06.21261707
- 18 Yellow Card
- 19 The Evidence-Based Medicine Consultancy June 9, 2021
The Bombshell Outbreak in the Wuhan Lab
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2021/09/11/covid-19-lab-leak-report.aspx
Analysis by Dr. Joseph Mercola Fact Checked September 11, 2021
STORY AT-A-GLANCE
- The House Foreign Affairs Committee reviewed public and classified intelligence to reach their stunning conclusions that the virus did originate in the Wuhan Institute of Virology (WIV), and it was genetically manipulated
- Unfortunately, the mainstream media have ignored the report, providing even more evidence experts are hoping to manipulate what you know and what you do
- Evidence clearly points to a viral leak from the Wuhan lab before September 12, 2019, the date a public database of 22,000 viral samples from WIV was inexplicably taken offline
- In September and October daily volume at local hospitals was higher than in the past 2.5 years, and researchers found a much higher than average number of searches for COVID symptoms on the Chinese search engine, Baidu
- The Committee also concluded there was enough evidence to show genetic modification was viable, that new processes could produce genetic sequencing “indistinguishable from wild type” and that Peter Daszak likely has information about the specific gain-of-function research and should be brought to testify before Congress
Any question about the origin of SARS-CoV-2 has been dispelled by a new addendum from the House Foreign Affairs Committee of the 117th Congress that reviewed public data and classified intelligence to reveal key new facts.1
In the short video above, Saagar Enjeti talks about a few of the interesting facts revealed in the addendum.2 Unfortunately, as has been the case throughout the last 18 months, the mainstream media completely ignored any report like this one, that suggests health experts have been manipulating what you see.
I believe it’s important to share information from the committee’s report with your friends and family as it sheds light on the lies the media have been perpetuating throughout 2020 and 2021. As you will see, and can find in the report, much of the information that led to the conclusions was taken from publicly available data.
If the media’s aim were to ferret out the truth and inform the public, this report may never have been necessary. And, if the media haven’t been telling you the truth about the origins of the virus, what else have they been hiding?
A report by the House Foreign Affairs Committee published in September 2020 highlighted the potential that SARS-CoV-2 was leaked from the Wuhan Institute of Virology (WIV). However, after discovering further evidence, the committee finds it is “time to completely dismiss the wet market as the source of the outbreak.”3
In the last 18 months, the virus has wreaked havoc on a health care system unwilling to use cost-effective and successful treatment modalities,4 and we have an economy that is still reeling from months of lockdowns and social distancing.
People are being forced to either accept the consequences and repercussions of hospital treatment for the infection or seek out successful alternatives that are criticized and discouraged by health agencies.5,6 If successful treatment were truly the objective, why would health experts vilify the use of medications that have been on the market for decades7,8 and the media maintain the lie?
Whether you are interested in the origin of a virus technocrats are using to manipulate human behavior or not, as Enjeti succinctly put it, “Getting to the bottom of it [origin of the pandemic] is vitally important for mankind so we can avoid any of this in the future.” And by “any of this” I take it to mean society’s complete trust in a system that has failed the public.
The Most Stunning Headline: Virus Was Leaked From the Lab
Enjeti believes the most stunning headline of the report is that the committee is convinced the virus was leaked from the lab,9 but that’s just the tip of the iceberg. The committee used publicly available data, intelligence reports and geospatial tracking to make their determination.
It appears the original infections likely occurred well before the December announcement from Wuhan, China. It is important to note that Wuhan is a large metropolitan city, home to some of the tallest skyscrapers, major cultural sites and multiple universities. As noted in the report, it is five times the size of Houston in land mass with a larger population than Chicago and New York City combined.10
Before the leak in 2019, the committee noted there had been several safety concerns in labs across the People’s Republic of China (PRC) since 2004. It was at this time that SARS leaked for the Beijing lab, and since then other accidental releases have occurred. From what the committee can discern, it is highly probable that SARS-CoV-2 was released from the Wuhan lab before September 12, 2019.
It was that date, September 12, 2019, that the online public database WIV of viral sequences and samples disappeared. The database had more than 22,000 entries of pathogens collected from mice and bats, with key information including similarities to other known viruses.
Dr. Shi Zheng-li was the senior scientist at WIV who was listed as the data correspondence author, but as the report highlights, to date has not given a consistent answer as to why the online database was removed or when or if it will be put back online.
Coincidentally, researchers from Harvard Medical School and Boston University School of Public Health had been evaluating 2.5 years of satellite imagery of hospitals in Wuhan.11 They were analyzing parking lot traffic volume and discovered that in September and October 2019, five of the six hospitals in the city had volume that was much higher than in the previous 2.5 years.
The researchers found this peak correspondent with a higher number of searches for two central COVID symptoms — “cough” and “diarrhea” — on the Chinese search engine Baidu.
Was the 2019 Military Games the Ultimate Superspreader?
Each of these factors and more identified in the report, point to the likelihood the virus had been released from the lab before September 12, 2019. Data gathered after the 2019 Military World Games held in Wuhan October 18, 2019, further support the committee’s assertion that the virus may have been contained to a local outbreak had truth been told.12
The military games are an Olympic-style event that drew 9,308 athletes from 109 countries, including the U.S.13,14 There were 25 countries that sent more than 100 athletes. The government used 236,000 volunteers, 90 hotels and more than 2,000 drivers. In other words, the games were a hotbed for spreading around the world what could have been contained as a local virus.
One journalist from the Financial Post15 reported some participants at the games described Wuhan as a “ghost town.” One of the athletes told the reporter, “This was a city of 15 million people that was in lockdown. It was strange, but we were told this was to make it easy for the games’ participants to get around.”16
The source shared there were 60 Canadian athletes put in isolation on the flight home who had symptoms of coughing and diarrhea. Once home, he reported that the symptoms became worse and included nosebleeds, fever and pain with breathing. Family members became ill and doctors were unable to identify a source for the infection. Another military source reported:17
“One-quarter of us got sick, there and when we returned. Some were bedridden for weeks. This made us potential vectors for the virus. The military did nothing. I was sick and others were, too, with Wuhan symptoms … I was eventually given a swab test, which measures only recent exposure, and told to carry on.”
The committee identified four countries that had sent athletes to the games that had people with confirmed COVID-19 in November and December 2019.18 Those countries were Italy, Brazil, Sweden and France. In both Italy and France, the individuals infected had no known history of traveling outside the country. This suggests the virus was brought into the country from another source. The Committee concluded:19
“While much of the public debate was initially focused on the Huanan seafood market in Wuhan as the origin of the pandemic, the preponderance of evidence now suggests that the virus leaked from the Wuhan Institute of Virology.
Given the WIV’s demonstrated history of conducting gain-of-function experiments on coronaviruses, including genetically manipulating viruses specifically to make them infectious to humans in BSL-2 labs, as well as their possession of one of the world’s largest collections of coronaviruses, it is completely plausible that one or more researcher(s) was accidentally infected and carried the virus out of the lab.”
Committee Also Believes the Virus Was Genetically Modified
Twenty-nine pages into the report, the committee began addressing the topic of genetic modification. Within the first paragraph they said there was enough evidence to suggest that genetic modification is a “viable hypothesis.”20 The committee included research from a 16-year collaboration between Peter Daszak, president of EcoHealth Alliance, and Dr. Shi Zheng-li, senior scientist at WIV, which revealed a strong relationship. They wrote:21
“Beginning in 2005, and continuing over the next 16 years, Shi and Daszak have collaborated on coronavirus research. Together, they ‘led dozens of expeditions to caves full of bats, to collect samples and analyze them.’
They have identified more than 500 novel coronaviruses, including roughly 50 related to SARS or MERS, and they have repeatedly engaged in gain-of-function research on coronaviruses designed to make them more infectious in humans.”
Information from the papers they co-wrote also appears in the committee report, three of which were papers on bat SARS-like coronaviruses. The paper in 2013 that was published in the journal Nature was called “Isolation and characterization of a bat SARS-like coronavirus that uses the ACE2 receptor.”22
In 2015, Shi gave Ralph Baric and researchers at the University of North Carolina Chapel Hill spike protein sequences and plasmids they identified from bat feces samples in 2013. The Committee reported these were used by American researchers to create:23
“’… a chimeric virus expressing the spike of bat coronavirus SHC014 in a mouse-adapted SARS-CoV backbone.’ In other words, they removed the spike protein from SHC014 and inserted it into a SARS coronavirus that was genetically manipulated to better infect mice.”
The research was funded by the NIAID and the NIH through the EcoHealth Alliance and the PRC government. In a paper published in 2016, in which Baric was the corresponding author, the writers discussed “moving from disease surveillance to creating chimeric viruses as a means of pandemic preparedness.”24 After reviewing the data, the committee concluded:
“Given the above, it is self-evident that Shi and her colleagues, with funding and support from Daszak, were actively genetically manipulating coronaviruses and testing them against human immune systems in 2018 and 2019, before the beginning of the pandemic.”
The committee’s report delved further into some of the unusual features of the SARS-CoV-2 virus. They point out that critics claim what they say is an apparent “lack of telltale signs of genetic manipulation” is proof that the virus is naturally occurring.
However, Baric had developed and published a novel genetic engineering system to allow for genetic sequencing that would create a new and infectious coronavirus that was “indistinguishable from wild type.”
Daszak’s Dark Relationship With Wuhan
Daszak is the only scientist named in the Executive Summary of the report and whose actions “call into question the way in which U.S. government grants are used in overseas labs and call for more oversight of those grants.”25 To understand the full implications of emails connecting Fauci and Daszak in early 2020, it’s important to understand what happened in the days before.
At the GOP House Oversight and Reform Subcommittee, Rep. Jim Jordan, R-Ohio, shared email information revealed in a Freedom of Information Act release, which demonstrated Fauci and many other health experts in the world knew the virus was lab-created.26
Jordan quotes from an email Fauci received from British researcher Christian Anderson that said, “The unusual features of the virus make up a really small part of the genome so one has to look really closely at all the sequences to see that some of the features look engineered. Eddie, Bob, Mike and myself all find the genome inconsistent with expectations from evolutionary theory.”27
In a separate presentation at the House Select Committee on the Coronavirus, Jordan illustrated Fauci’s changing narrative on the issue of gain-of-function research, which is a lab-performed genetic alteration to make a virus more infectious to humans, saying:28
“He initially said the United States taxpayer money did not fund the Wuhan Institute of Virology. He later changed that, saying no, no we did fund it but it was through a sub-grant. He subsequently said no, no we funded it but we did not fund gain-of-function research.
Then just last Sunday he said, well, we funded it, there was gain-of-function research, but it was a sound scientific decision. And then he said this … it would have been negligent to not fund the lab in China.”
In a section of the report from the House Foreign Affairs Committee titled “The Cover Up,”29 there is evidence that Daszak pushed for a cover up. His actions included bullying scientists who asked questions and directly lying about the nature of the research and about the low-level safety protocols being used in the research. They conclude his actions cost time and “provide further proof the virus likely leaked from the WIV.”30
Daszak Grateful Fauci on Board With Cover Up
In April 2020, Fauci was at the White House, where he rejected the idea that the coronavirus was created in the lab in Wuhan.31 In July 2020, Daszak headed up a second commission to investigate the origin of the virus, The Lancet COVID-19 commission,32 despite his many conflicts of interest and of having openly and repeatedly dismissed the possibility of the pandemic being the result of a lab leak.33
However, once Fauci’s emails were released under a Freedom of Information Act request, it was discovered that Daszak wrote: “I just wanted to say a personal thank you on behalf of our staff and collaborators, for publicly standing up and stating that the scientific evidence supports a natural origin for COVID-19 from a bat-to-human spillover, not a lab release from the Wuhan Institute of Virology.”34
Jordan quotes testimony from “Dr. Jarrar,” whom he identifies as a former assistant secretary for health, that supports the mounting evidence being revealed. Jordan said:35
“Here’s what Dr. Jarrar said. ‘I believe it’s just too much of a coincidence that the worldwide pandemic caused by a novel bat coronavirus that cannot be found in nature started just a few miles away from a secretive laboratory doing potentially dangerous research on bat coronaviruses.'”
In the House Committee’s report, Daszak’s name is mentioned 125 times. The importance of Daszak’s position in gain-of-function research done at WIV and the ensuing coverup is brought home by the committee’s recommendation for the next steps that Congress should take, namely “After this extensive investigation, we believe it is time to call Peter Daszak to testify before Congress.”36
- 1, 3, 10, 12, 13, 18, 20, 21, 23, 24, 25 House Foreign Affairs Committee Report, Minority Staff, August 2021
- 2 YouTube, August 5, 2021
- 4 FLCCC.net
- 5 FDA, July 1, 2020
- 6 NIH, February 11, 2021
- 7 Lupus Foundation of America, Hydroxychloroquine 1956
- 8 IS Global, November 21, 2019
- 9 YouTube, August 5, 2021, Min 00:36
- 11 Digital Access to Scholarship at Harvard, Analysis of hospital traffic
- 14 US Department of Defense, 7th International Military Sports Council
- 15, 16, 17 Financial Post, June 25, 2021
- 19 House Foreign Affairs Committee Report, Minority Staff, August 2021, Conclusion page 29
- 22 Nature, 2013; 503
- 26, 28 YouTube, June 29, 2021
- 27 YouTube, June 29, 2021, Minute 00:12
- 29, 30, 36 House Foreign Affairs Committee Report, Minority Staff, August 2021
- 31 Insider, April 18, 2020
- 32 The Lancet October 10, 2020; 396(10257): 1102
- 33 GM Watch September 23, 2020
- 34 KATV, June 3, 2021
- 35 YouTube, July 28, 2021, Minute 3:15
A ‘Leap’ Toward Humanity’s Destruction
Reproduced from original article:
https://articles.mercola.com/sites/articles/archive/2021/08/17/a-leap-toward-humanitys-destruction.aspx
Analysis by Whitney Webb August 17, 2021

This article originally appeared on Unlimited Hangout.
The world’s richest medical research foundation, the Wellcome Trust, has teamed up with a pair of former DARPA directors who built Silicon Valley’s skunkworks to usher in an age of nightmarish surveillance, including for babies as young as three months old. Their agenda can only advance if we allow it.
A UK nonprofit with ties to global corruption throughout the COVID-19 crisis as well as historical and current ties to the UK eugenics movement launched a global health-focused DARPA equivalent last year. The move went largely unnoticed by both mainstream and independent media.
The Wellcome Trust, which has arguably been second only to Bill Gates in its ability to influence events during the COVID-19 crisis and vaccination campaign, launched its own global equivalent of the Pentagon’s secretive research agency last year, officially to combat the “most pressing health challenges of our time.”
Though first conceived of in 2018, this particular Wellcome Trust initiative was spun off from the Trust last May with $300 million in initial funding. It quickly attracted two former DARPA executives, who had previously served in the upper echelons of Silicon Valley, to manage and plan its portfolio of projects.
This global health DARPA, known as Wellcome Leap, seeks to achieve “breakthrough scientific and technological solutions” by or before 2030, with a focus on “complex global health challenges.” The Wellcome Trust is open about how Wellcome Leap will apply the approaches of Silicon Valley and venture capital firms to the health and life science sector.
Unsurprisingly, their three current programs are poised to develop incredibly invasive tech-focused, and in some cases overtly transhumanist, medical technologies, including a program exclusively focused on using artificial intelligence (AI), mobile sensors, and wearable brain-mapping tech for children three years old and younger.
This Unlimited Hangout investigation explores not only the four current programs of Wellcome Leap but also the people behind it. The resulting picture is of an incredibly sinister project that poses not only a great threat to current society but to the future of humanity itself. An upcoming Unlimited Hangout investigation will examine the history of the Wellcome Trust along with its role in recent and current events.
Leap’s Leadership: Merging Man and Machine for the Military and Silicon Valley
The ambitions of the Wellcome Leap are made clear by the woman chosen to lead it, former director of the Pentagon’s DARPA, Regina Dugan. Dugan began her career at DARPA in 1996; she led a counterterrorism task force in 1999 before leaving DARPA about a year later.
After departing DARPA, she cofounded her own venture capital firm, Dugan Ventures, and then became special adviser to the US Army’s vice chief of staff from 2001 to 2003, which coincided with the invasions of Afghanistan and Iraq. In 2005, she created a defense-focused tech firm called RedXDefense, which contracts with the military and specifically for DARPA.
In 2009, under the Obama administration, Dugan was appointed director of DARPA by Defense Secretary Robert Gates. Much was made over her being the first female director of the agency, but she is best remembered at the agency for her so-called “Special Forces” approach to innovation. During her tenure, she created DARPA’s now defunct Transformational Convergence Technology Office, which focused on social networks, synthetic biology, and machine intelligence.
Many of the themes previously managed by that office are now overseen by DARPA’s Biological Technologies Office, which was created in 2014 and focuses on everything “from programmable microbes to human-machine symbiosis.” The Biological Technologies Office, like Wellcome Leap, pursues a mix of “health-focused” biotechnology programs and transhumanist endeavors.
Right before leaving the top role at DARPA, Dugan greenlighted the agency’s initial investments in mRNA vaccine technology, which led to DARPA’s investments in Pfizer and Moderna shortly thereafter. The DARPA scientist who lobbied Dugan to back the program, Dan Wattendorf, now works as the director of Innovative Technology Solutions at the Bill & Melinda Gates Foundation.
While Dugan’s efforts at DARPA are remembered fondly by those in the national-security state, and also by those in Silicon Valley, Dugan was investigated for conflicts of interest during her time as DARPA’s director, as her firm RedXDefense acquired millions in Department of Defense contracts during her tenure.
Though she had recused herself from any formal role at the company while leading DARPA, she continued to hold a significant financial stake in the company, and a military investigation later found she had violated ethics rules to a significant degree.
Instead of being held accountable in any way, Dugan went on to become a top executive at Google, where she was brought on to manage Google’s Advanced Technology and Products Group (ATAP), which it had spun out of Motorola Mobility after Google’s acquisition of that company in 2012. Google’s ATAP was modeled after DARPA and employed other ex-DARPA officials besides Dugan.
At Google, Dugan oversaw several projects, including what is now the basis of Google’s “augmented reality” business, then known as Project Tango, as well as “smart” clothing in which multitouch sensors were woven into textiles. Another project that Dugan led involved the use of a “digital tattoo” to unlock smartphones. Perhaps most controversially, Dugan was also behind the creation of a “digital authentication pill.”
According to Dugan, when the pill is swallowed, “your entire body becomes your authentication token.” Dugan framed the pill and many of her other efforts at Google as working to fix “the mechanical mismatch between humans and electronics” by producing technology that merges the human body with machines to varying degrees.
While serving in this capacity at Google, Dugan chaired a panel at the 2013 Clinton Global Initiative called “Game-Changers in Technology” and attended the 2015 Bilderberg meeting where AI was a main topic of discussion.
In 2016, Dugan left Google for Facebook where she was chosen to be the first head of Facebook’s own DARPA-equivalent research agency, then known as Building 8. DARPA’s ties to the origins of Facebook were discussed in a recent Unlimited Hangout report.
Under Dugan, Building 8 invested heavily in brain-machine interface technology, which has since produced the company’s “neural wearable” wristbands that claim to be able to anticipate movements of the hand and fingers from brain signals alone. Facebook showcased prototypes of the project earlier this year.
Dugan left Facebook just eighteen months after joining Building 8, announcing her plans “to focus on building and leading a new endeavor,” which was apparently a reference to Wellcome Leap. Dugan later said it was as if she had been training for her role at Wellcome Leap ever since entering the workforce, framing it as the pinnacle of her career.
When asked in an interview earlier this year who the clients of Wellcome Leap are, Dugan gave a long-winded answer but essentially responded that the project serves the biotech and pharmaceutical industries, international organizations such as the UN, and public-private partnerships.
In addition to her role at Wellcome, Dugan is also a member of the Council on Foreign Relations-sponsored taskforce on US Technology and Innovation policy, which was formed in 2019. Other members include LinkedIn’s Reid Hoffman, McKinsey Institute Global Chairman James Manyika, former head of Google Eric Schmidt and President Biden’s controversial top science adviser Eric Lander.
The other executive at Wellcome Leap, chief operating officer Ken Gabriel, has a background closely tied to Dugan’s. Gabriel, like Dugan, is a former program manager at DARPA, where he led the agency’s microelectromechanical systems (MEMS) research from 1992 to 1996.
He served as deputy director of DARPA from 1995 to 1996 and became director of the Electronics Technology Office from 1996 to 1997, where he was reportedly responsible for about half of all federal electronics-technology investments. At DARPA, Gabriel worked closely with the FBI and the CIA.

Gabriel left DARPA for Carnegie Mellon University, where he was in charge of the Office for Security Technologies in the aftermath of September 11, 2001. That office was created after 9/11 specifically to help meet the national-security needs of the federal government, according to Carnegie Mellon’s announcement of the program.
Around that same time, Gabriel became regarded as “the architect of the MEMS industry” due to his past work at DARPA and his founding of the MEMS-focused semiconductor company Akustica in 2002. He served as Akustica’s chairman and chief technology officer until 2009, at which time he returned to work at DARPA where he served as the agency’s deputy director, working directly under Regina Dugan.
In 2012, Gabriel followed Dugan to Google’s Advanced Technology and Products Group, which he was actually responsible for creating. According to Gabriel, Google cofounders Larry Page and Sergey Brin tasked Gabriel with creating “a private sector ground-up model of DARPA” out of Motorola Mobility. Regina Dugan was placed in charge, and Gabriel again served as her deputy.
In 2013, Dugan and Gabriel co-wrote a piece for the Harvard Business Review about how DARPA’s “Special Forces” innovation approach could revolutionize both the public and private sectors if more widely applied.
Gabriel left Google in 2014, well before Dugan, to serve as the president and CEO of Charles Stark Draper Laboratories, better known as Draper Labs, which develops “innovative technology solutions” for the national-security community, with a focus on biomedical systems, energy, and space technology. Gabriel held that position until he abruptly resigned in 2020 to co-lead Wellcome Leap with Dugan.
In addition to his role at Wellcome, Gabriel is also a World Economic Forum “technology pioneer” and on the board of directors of Galvani Bioelectronics, a joint venture of GlaxoSmithKline, which is intimately linked to the Wellcome Trust, and the Google subsidiary Verily.
Galvani focuses on the development of “bioelectronic medicines” that involve “implant-based modulation of neural signals” in an overt push by the pharmaceutical industry and Silicon Valley to normalize transhumanist “medicines.”
The longtime chairman of the board of Galvani, on which Gabriel serves, was Moncef Slaoui, who led the US COVID-19 vaccine development and distribution program Operation Warp Speed. Slaoui was relieved of his position at Galvani this past March over well-substantiated claims of sexual harassment.
Jeremy Farrar, Pandemic Narrative Manager
While Dugan and Gabriel ostensibly lead the outfit, Wellcome Leap is the brainchild of Jeremy Farrar and Mike Ferguson, who serve as its directors. Farrar is the director of the Wellcome Trust itself, and Ferguson is deputy chair of the Trust’s board of governors.
Farrar has been director of the Wellcome Trust since 2013 and has been actively involved in critical decision making at the highest level globally since the beginning of the COVID crisis. He is also an agenda contributor to the World Economic Forum and cochaired the WEF’s Africa meeting in 2019.
Farrar’s Wellcome Trust is also a WEF strategic partner and cofounded the COVID Action Platform with the WEF. Farrar was more recently behind the creation of Wellcome’s COVID-Zero initiative, which is also tied to the WEF.
Farrar has framed that initiative as “an opportunity for companies to advance the science which will eventually reduce business disruption.” Thus far it has convinced titans of finance, including Mastercard and Citadel, to invest millions in research and development at organizations favored by the Wellcome Trust.

Source: NTI.com
Some of Wellcome’s controversial medical-research projects in Africa, as well as its ties to the UK eugenics movement, were explored in a December article published at Unlimited Hangout.
That report also explores the intimate connections of Wellcome to the Oxford-AstraZeneca COVID-19 vaccine, the use of which has now been restricted or banned in several countries. As mentioned in the introduction, the Wellcome Trust itself is the subject of an upcoming Unlimited Hangout investigation (Part 2).
Jeremy Farrar, who was born in Singapore in 1961, had previously been director of the Oxford University Clinical Research Unit in Ho Chi Minh City, beginning in 1998. During that time, he authored numerous epidemiological research papers. He claimed in a 2014 Financial Times article that his decision to move to Vietnam was due to his disdain for conference halls full of white men.
Southeast Asia was obviously a much less regulated environment for someone in the medical-research industry wishing to indulge in groundbreaking research. Although based in Vietnam, Farrar was sent by Oxford to various locations around the globe to study epidemics happening in real time.
In 2009, when swine flu was wreaking havoc in Mexico, Farrar jumped on a plane to dive right into the action, something he also did for subsequent global outbreaks of Ebola, MERS, and avian flu.
Over the past year, many questions have arisen regarding exactly how much power Farrar wields over global public health policy. Recently, the US president’s chief medical adviser, Anthony Fauci, was forced to release his emails and correspondence from March and April 2020 at the request of the Washington Post.
The released emails reveal what appears to be a high-level conspiracy by some of the top medical authorities in the US to falsely claim that COVID-19 could only have been of zoonotic origin, despite indications to the contrary. The emails were heavily redacted as such emails usually are, supposedly to protect the information of the people involved, but the “(b)(6)” redactions also protect much of Jeremy Farrar’s input into these discussions.
Chris Martenson, economic researcher and post-doctorate student of neurotoxicology and founder of Peak Prosperity, has had some insightful comments on the matter, including asking why such protection has been offered to Farrar given that he is the director of a “charitable trust.” Martenson went on to question why the Wellcome Trust was involved at all in these high-level discussions.
One Fauci email, dated February 25, 2020, and sent by Amelie Rioux of the WHO, stated that Jeremy Farrar’s official role at that time was “to act as the board’s focal point on the COVID-19 outbreak, to represent and advise the board on the science of the outbreak and the financing of the response.”
Farrar had previously chaired the WHO’s Scientific Advisory Council. The emails also show the preparation, within a ten-day period, of the SARS-CoV-2 “‘origins” paper, which was entitled “The Proximal Origin of SARS-CoV-2” and was accepted for publication by Nature Medicine on March 17, 2020.
The paper claimed that the SARS-CoV-2 virus could only have come from natural origins as opposed to gain-of-function research, a claim once held as gospel in the mainstream but which has come under considerable scrutiny in recent weeks.
Shaping the presentation of an origin story for a virus of global significance is something Farrar has been involved with before. In 2004–5, it was reported that Farrar and his Vietnamese colleague Tran Tinh Hien, the vice director at the Hospital for Tropical Diseases, were the first to identify the re-emergence of the avian flu (H5N1) in humans.
Farrar has recounted the origin story on many occasions, stating: “It was a little girl. She caught it from a pet duck that had died and she’d dug up and reburied. She survived.” According to Farrar, this experience prompted him to found a global network in conjunction with the World Health Organization to “improve local responses to disease outbreaks.”
An article published by Rockefeller University Press’s Journal of Experimental Medicine in 2009 is dramatically titled, “Jeremy Farrar: When Disaster Strikes.” Farrar, when referring to the H5N1 origin story stated: “The WHO people—and this is not a criticism—decided it was unlikely that the child had SARS or avian influenza.
They left, but Professor Hien stayed behind to talk with the child and her mum. The girl admitted that she had been quite sad in the previous days with the death of her pet duck. The girl and her brother had fought over burying the duck and, because of this argument, she had gone back, dug up the duck, and reburied it—probably so her brother wouldn’t know where it was buried.
With that history, Professor Hien phoned me at home and said he was worried about the child. He took some swabs from the child’s nose and throat and brought them back to the hospital. That night the laboratory ran tests on the samples, and they were positive for Influenza A.”
With Farrar now having been revealed as an instrumental part of the team that crafted the official story regarding the origins of SARS-CoV-2, his previous assertions about the origin of past epidemics should be scrutinized.
As the director of a “charitable trust,” Jeremy Farrar is almost completely unaccountable for his involvement in crafting controversial narratives related to the COVID crisis. He continues to be at the forefront of the global response to COVID, in part by launching the Wellcome Leap Fund for “unconventional projects, funded at scale” as an overt attempt to create a global and “charitable” version of DARPA.
Indeed, Farrar, in conceiving Wellcome Leap, has positioned himself to be just as, if not more, instrumental in building the foundation for the post-COVID era as he was in building the foundation for the COVID crisis itself.
This is significant as Wellcome Leap CEO Regina Dugan has labeled COVID-19 this generation’s “Sputnik moment” that will launch a new age of “health innovation,” much like the launching of Sputnik started a global technological “space age.” Wellcome Leap fully intends to lead the pack.
“Rulers” of the Gene-Sequencing Industry
In contrast to the overt DARPA, Silicon Valley, and Wellcome connections of the others, the chairman of the board of directors of Wellcome Leap, Jay Flatley, has a different background. Flatley is the long-time head of Illumina, a California-based gene-sequencing hardware and software giant that is believed to currently dominate the field of genomics.
Though he stepped down from the board of Illumina in 2016, he has continued to serve as the executive chairman of its board of directors. Flatley was the first to be chosen for a leadership position at Wellcome Leap, and he was responsible for suggesting Regina Dugan for the organization’s chief executive officer, according to a recent interview given by Dugan.

As a profile on Illumina in the business magazine Fast Company notes, Illumina “operates behind the scenes, selling hardware and services to companies and research institutions,” among them 23andMe. 23andMe’s CEO, Anne Wojcicki, the sister of YouTube CEO Susan Wojcicki and the wife of Google cofounder Sergey Brin, told Fast Company, “It’s crazy. Illumina is like the ruler of this whole universe and no one knows that.”
The report notes that 23andMe, like most companies that offer DNA sequencing and analysis to consumers, uses machines produced by Illumina.
In 2016, Illumina launched an “aggressive” five-year plan to “bring genomics out of research labs and into doctors’ offices.” Given the current state of things, particularly the global push toward gene-focused vaccines and therapies, that plan, which concludes this year, could not have been any better timed.
Illumina’s current CEO, Francis DeSouza, previously held key posts at Microsoft and Symantec. Also in 2016, Illumina’s executive teams forecast a future in which humans are gene tested from birth to grave for both health and commercial purposes.
Whereas most companies have struggled financially during the coronavirus pandemic, some have seen a massive increase in profits. Illumina has witnessed its share price double since the start of the COVID crisis.
The company’s $1 billion plus in profits during the last tax year was obviously helped by the quick approval of the NovaSEQ 6000 machines, which can test a large number of COVID samples more quickly than other devices. An individual machine has a hefty price tag of almost $1 million, and thus they are mostly found at elite facilities, private labs, and top-tier universities.
 Jay Flatley, Executive Chairman, Illumina, speaking at World Economic Forum in Davos 2018. Source: WEF
Jay Flatley, Executive Chairman, Illumina, speaking at World Economic Forum in Davos 2018. Source: WEFIn addition to his long-standing leadership role at Illumina, Jay Flatley is also a “digital member” of the World Economic Forum as well as the lead independent director of Zymergen, a WEF “tech pioneer” company that is “rethinking biology and reimagining the world.”
Flatley, who has also attended several Davos meetings, has addressed the WEF on the “promise of precision [i.e., gene-specific] medicine.”
At another WEF panel meeting, Flatley, alongside UK Health Secretary Matt Hancock, promoted the idea of making genomic sequencing of babies at birth the norm, claiming it had “the potential to shift the healthcare system from reactive to preventative.”
Some at the panel called for the genomic sequencing of infants to eventually become mandatory.
Aside from Flatley as an individual, Illumina as a company is a WEF partner and plays a key role in its platform regarding the future of health care. A top Illumina executive also serves on the WEF’s Global Future Council on Biotechnology.
A New HOPE
Wellcome Leap currently has four programs: Multi-Stage Psych, Delta Tissue, 1KD, and HOPE. HOPE was the first program to be announced by Wellcome Leap and stands for Human Organs, Physiology and Engineering. According to the full program description, HOPE aims “to leverage the power of bioengineering to advance stem cells, organoids, and whole organ systems and connections that recapitulate human physiology in vitro and restore vital functions in vivo.”
HOPE consists of two main program goals. First, it seeks to “bioengineer a multiorgan platform that recreates human immunological responses with sufficient fidelity to double the predictive value of a preclinical trial with respect to efficacy, toxicity and immunogenicity for therapeutic interventions.”
In other words, this bioengineered platform mimicking human organs would be used to test the effects of pharmaceutical products, including vaccines, which could create a situation in which animal trials are replaced with trials on gene-edited and farmed organs.
Though such an advance would certainly be helpful in the sense of reducing often unethical animal experimentation, trusting such a novel system to allow medical treatments to go straight to the human-testing phase would also require trusting the institutions developing that system and its funders.
As it stands now, the Wellcome Trust has too many ties to corrupt actors in the pharmaceutical industry, having originally begun as the “philanthropic” arm of UK drug giant GlaxoSmithKline, for anyone to trust what they are producing without actual independent confirmation, given the histories of some of their partners in fudging both animal and human clinical trial data for vaccines and other products.
The second goal of HOPE is to open up the use of machine-human hybrid organs for transplantation into human beings. That goal focuses on restoring “organ functions using cultivated organs or biological/synthetic hybrid systems” with the later goal of bioengineering a fully transplantable human organ after several years.
Later on in the program description, however, the interest in merging the synthetic and biological becomes clearer when it states: “The time is right to foster synergies between organoids, bioengineering and immunoengineering technologies, and advance the state-of-the-art of in vitro human biology … by building controllable, accessible and scalable systems.”
The program description document also notes the interest of Wellcome in genetic-engineering approaches for the “enhancement of desired properties and insertion of traceable markers” and Wellcome’s ambition to reproduce the building blocks of the human immune system and human organ systems through technological means.
Transhumanist Toddlers?
The second program to be pursued by Wellcome Leap is called “The First 1000 Days: Promoting Healthy Brain Networks,” which is abbreviated as 1KD by the organization. It is arguably the most unsettling program because it seeks to use young children, specifically infants from three months to three-year-old toddlers, as its test subjects.
The program is being overseen by Holly Baines, who previously served as strategy development lead for the Wellcome Trust before joining Wellcome Leap as the 1KD program leader.
1KD is focused on developing “objective, scalable ways to assess a child’s cognitive health” by monitoring the brain development and function of infants and toddlers, allowing practitioners to “risk-stratify children” and “predict responses to interventions” in developing brains.
The program description document notes that, up to this point in history, “our primary window into the developing brain has been neuroimaging techniques and animal models, which can help identify quantitative biomarkers of [neural] network health and characterise network differences underlying behaviours.” It then states that advances in technology “are opening additional possibilities in young infants.”
The program description goes on to say that artificial neural networks, a form of AI, “have demonstrated the viability of modelling network pruning process and the acquisition of complex behaviours in much the same way as a developing brain,” while improvements in machine learning, another subset of AI, can now be used to extract “meaningful signals” from the brains of infants and young children.
These algorithms can then be used to develop “interventions” for young children deemed by other algorithms to be in danger of having underdeveloped brain function.
The document goes on to note the promise of “low-cost mobile sensors, wearables and home-based systems” in “providing a new opportunity to assess the influence and dependency of brain development on natural physical and social interactions.”
In other words, this program seeks to use “continuous visual and audio recordings in the home” as well as wearable devices on children to collect millions upon millions of data points. Wellcome Leap describes these wearables as “relatively unobtrusive, scalable electronic badges that collect visual, auditory and motion data as well as interactive features (such as turn-taking, pacing and reaction times).”
Elsewhere in the document there is a call to develop “wearable sensors that assess physiological measures predictive of brain health (e.g., electrodermal activity, respiratory rate, and heart rate) and wireless wearable EEG or eye-tracking technology” for use in infants and children three and under.
Like other Wellcome Leap programs, this technology is being developed with the intention of making it mainstream in medical science within the next five to ten years, meaning that this system—although framed as a way to monitor children’s brain functioning to improve cognitive outcomes—is a recipe for total surveillance of babies and very young children as well as a means for altering their brain functioning as algorithms and Leap’s programmers see fit.
1DK has two main program goals. The first is to “develop a fully integrated model and quantitive measurement tools of network development in the first 1000 days [of life], sufficient to predict EF [executive function] formation before a child’s first birthday.”
Such a model, the description reads, “should predict contributions of nutrition, the microbiome and the genome” on brain formation as well as the effects of “sensimotor and social interactions [or lack thereof] on network pruning processes” and EF outcomes. The second goal makes it clear that widespread adoption of such neurological-monitoring technologies in young children and infants is the endgame for 1DK.
It states that the program plans to “create scalable methods for optimising promotion, prevention, screening and therapeutic interventions to improve EF by at least 20% in 80% of children before age 3.”
True to the eugenicist ties of the Wellcome Trust (to be explored more in-depth in Part 2), Wellcome Leap’s 1DK notes that “of interest are improvements from underdeveloped EF to normative or from normative to well-developed EF across the population to deliver the broadest impact.”
One of the goals of 1DK is thus not treating disease or addressing a “global health public challenge” but instead experimenting on the cognitive augmentation of children using means developed by AI algorithms and invasive surveillance-based technology.
Another unsettling aspect of the program is its plan to “develop an in vitro 3D brain assembloid that replicates the time formation” of a developing brain that is akin to the models developed by monitoring the brain development of infants and children.
Later on, the program description calls this an “in-silico” model of a child’s brain, something of obvious interest to transhumanists who see such a development as a harbinger of the so-called singularity.
Beyond that, it appears that this in-silico and thus synthetic model of the brain is planned to be used as the “model” to which infant and children brains are shaped by the “therapeutic interventions” mentioned elsewhere in the program description.
It should be clear how sinister it is that an organization that brings together the worst “mad scientist” impulses of both the NGO and military-research worlds is openly planning to conduct such experiments on the brains of babies and toddlers, viewing them as datasets and their brains as something to be “pruned” by machine “intelligence.”
Allowing such a program to advance unimpeded without pushback from the public would mean permitting a dangerous agenda targeting society’s youngest and most vulnerable members to potentially advance to a point where it is difficult to stop.
A “Tissue Time Machine”
The third and second-most recent program to join the Wellcome Leap lineup is called Delta Tissue, abbreviated by the organization as ΔT. Delta Tissue aims to create a platform that monitors changes in human-tissue function and interactions in real time, ostensibly to “explain the status of a disease in each person and better predict how that disease would progress.”
Referring to this platform as a “tissue time machine,” Wellcome Leap sees Delta Tissue as being able to predict the onset of disease before it occurs while also allowing for medical interventions that “are targeted to the individual.”

Well before the COVID era, precision medicine or medicine “targeted or tailored to the individual” has been a code phrase for treatments based on patients’ genetic data and/or for treatments that alter nucleic acid (e.g., DNA and RNA) function itself. For instance, the US government defines “precision medicine” as “an emerging approach for disease treatment and prevention that takes into account individual variability in genes, environment, and lifestyle for each person.”
Similarly, a 2018 paper published in Technology notes that, in oncology, “precision and personalized medicine … fosters the development of specialized treatments for each specific subtype of cancer, based on the measurement and manipulation of key patient genetic and omic data (transcriptomics, metabolomics, proteomics, etc.).”
Prior to COVID-19 and the vaccine roll outs, the mRNA vaccine technology used by the DARPA-funded companies Moderna and Pfizer were marketed as being precision medicine treatments and were largely referred to as “gene therapies” in media reports.
They were also promoted heavily as a revolutionary method of treating cancer, making it unsurprising that the Delta Tissue program at Wellcome Leap would use a similar justification to develop a program that aims to offer tailored gene therapies to people before the onset of a disease.
This Delta Tissue platform works to combine “the latest cell and tissue profiling technologies with recent advances in machine learning,” that is, AI.
Given Wellcome Leap’s connections to the US military, it is worth noting that the Pentagon and Google, both former employers of Wellcome Leap CEO Regina Dugan and COO Ken Gabriel, have been working together since last September on using AI to predict disease in humans, first focusing on cancer before expanding to COVID-19 and every disease in between.
The Delta Tissue program appears to have related ambitions, as its program description makes clear that the program ultimately aims to use its platform for a host of cancers and infectious diseases.
The ultimate goal of this Wellcome Leap program is “to eradicate the stubbornly challenging diseases that cause so much suffering around the world.” It plans to do this through AI algorithms, however, which are never 100 percent accurate in their predictive ability, and with gene-editing treatments, nearly all of which are novel and have not been well tested.
That latter point is important given that one of the main methods for gene-editing in humans, CRISPR, has been found in numerous studies to cause considerable damage to the DNA, damage that is largely irreparable (see here, here and here).
It seems plausible that a person placed on such a hi-tech medical treatment path will continue to need a never-ending series of gene-editing treatments and perhaps other invasive hi-tech treatments to mitigate and manage the effects of clumsy gene splicing.
Total Surveillance to Treat “Depression”
Wellcome Leap’s most recent program, launched just this week, is called “Multi-Channel Psych: Revealing Mechanisms of Anhedonia” and is officially focused on creating “complex, biological” treatments for depression.

Those behind Wellcome Leap frame the problem they aim to tackle with this program as follows:
“We understand that synaptic connections serve as the currency of neural communication, and that strengthening or weakening these connections can facilitate learning new behavioral strategies and ways of looking at the world.
Through studies in both animal models and humans, we have discovered that emotional states are encoded in complex neural network activity patterns, and that directly changing these patterns via brain stimulation can shift mood. We also know that disruption of these delicately balanced networks can lead to neuropsychiatric illness.” (emphasis added)
They add that “biologically based treatments” for depression “are not being matched to the biology of the human beings they’re being used in,” and, thus, treatments for depression need to be tailored “to the specific biology” of individual patients. They clearly state that what needs to be addressed in order to make such personal modifications to treatment is to gain “easy access to the biological substrate of depression—i.e. the brain.”
Wellcome Leap’s program description notes that this effort will focus specifically on anhedonia, which it defines as “an impairment in the effort-based reward system” and as a “key symptom of depression and other neuropsychiatric illnesses.” Notably, in the fine print of the document, Wellcome Leap states:
“While there are many definitions of anhedonia, we are less interested in the investigation of reduced consummatory pleasure, the general experience of pleasure, or the inability to experience pleasure. Rather, as per the description above, we will prioritize investigations of anhedonia as it relates to impairments in the effort-based reward system—e.g. reduced motivation to complete tasks and decreased capacity to apply effort to achieve a goal.”
In other words, Wellcome Leap is only interested in treating aspects of depression that interfere with an individual’s ability to work, not in improving an individual’s quality or enjoyment of life.
Leap notes, in discussing its goals, that it seeks to develop models for how patients respond to treatments that include “novel or existing behavior modification, psychotherapy, medication, and neurostimulation options” while also capturing an individual’s “genome, phenome [the sum of an individual’s phenotypic traits], [neural] network connectivity, metabolome [the sum of an individual’s metabolic traits], microbiome, reward processing plasticity levels,” among others.
It ultimately aims to predict the relationship between an individual’s genome to how “reward processing” functions in the brain. It implies that the data used to create this model should involve the use of wearables, stating that researchers “should seek to leverage high frequency patient-worn or in-home measurements in addition to those obtained in the clinic, hospital or laboratory.”
One of the main research areas included in the program looks to “develop new scalable measurement tools for reliable and high-density quantification of mood (both subjectively reported and objectively quantified via biometrics such as voice, facial expression, etc.), sleep, movement, reward system functioning, effort/motivation/energy levels, social interaction, caloric intake, and HPA axis output in real-world situations.”
The HPA (hypothalamic-pituitary-adrenal) axis is mentioned throughout the document, and this is significant as it is both a negative and positive feedback system regulating the mechanisms of stress reactions, immunity, and also fertility in the human body.
The latter is especially important given the Wellcome Trust’s ties to the UK eugenics movement. It is also worth noting that some commercially available wearables, such as Amazon’s Halo, already quantify mood, sleep, and movement.
The program’s authors go even further than the above in terms of what they wish to monitor in real time, stating, “We specifically encourage the development of non-invasive technology to directly interrogate human brain state.” Examples include “a non-invasive spinal tap equivalent,” “behavioral or biomarker probes of neural plasticity,” and “single-session neural monitoring capabilities that define a treatment-predictive brain state.”
In other words, this Wellcome Leap program and its authors seek to develop “non-invasive” and, likely, wearable technology capable of monitoring an individual’s mood, facial expressions, social interactions, effort and motivation, and potentially even thoughts in order to “directly interrogate human brain state.”
To think that such a device would stay only in the realm of research is naive, especially given that WEF luminaries have openly spoken at Davos meetings about how governments plan to use such technology widely on their populations as a means of pre-emptively targeting would-be dissent and ushering in an era of “digital dictatorships.”
The focus on treating only the aspects of depression that interfere with a person’s work further suggests that such technology, once developed, would be used to ensure “perfect worker” behavior in industries where human workers are rapidly being replaced with AI and machines, meaning the rulers can be more selective about which people continue to be employed and which do not.
Like other Wellcome Leap programs, if completed, the fruits of the Multi-Channel Psych program will likely be used to ensure a population of docile automatons whose movements and thoughts are heavily surveilled and monitored.
The Last Leap for an Old Agenda
Wellcome Leap is no small endeavor, and its directors have the funding, influence, and connections to make their dreams reality. The organization’s leadership includes the key force behind Silicon Valley’s push to commercialize transhumanist tech (Regina Dugan), the “architect” of the MEMS industry (Ken Gabriel), and the “ruler” of the burgeoning genetic-sequencing industry (Jay Flatley).
It also benefits from the funding of the world’s largest medical-research foundation, the Wellcome Trust, which is also one of the leading forces in shaping genetics and biotechnology research as well as health policy globally.
A 1994 Sunday Times investigation into the Trust noted that “through [Wellcome Trust] grants and sponsorships, government agencies, universities, hospitals and scientists are influenced all over the world. The trust distributes more money to institutions than even the British government’s Medical Research Council.” It then notes:
“In offices on the building’s first floor, decisions are reached that affect lives and health on scales comparable with minor wars. In the conference room, high above the street, and in the meeting hall, in the basement, rulings in biotechnology and genetics are handed down that will help shape the human race.”
Little has changed regarding the Trust’s influence since that article was published. If anything, its influence on research paths and decisions that will “shape the human race” has only grown. Its ex-DARPA officials, who have spent their careers advancing transhumanist technology in both the public and private sectors, have overlapping goals with those off Wellcome Leap.
Dugan’s and Gabriel’s commercial projects in Silicon Valley reveal that Leap is led by those who have long sought to advance the same technology for profit and for surveillance. This drastically weakens Wellcome Leap’s claim to now be pursuing such technologies to only improve “global health.”
Indeed, as this report has shown, most of these technologies would usher in a deeply disturbing era of mass surveillance over both the external and internal activities of human beings, including young children and infants, while also creating a new era of medicine based largely on gene-editing therapies, the risks of which are considerable and also consistently downplayed by its promoters.
When one understands the intimate bond that has long existed between eugenics and transhumanism, Wellcome Leap and its ambitions make perfect sense. In a recent article written by John Klyczek for Unlimited Hangout, it was noted that the first director general of UNESCO and former president of the UK Eugenics Society was Julian Huxley, who coined the term “transhumanism” in his 1957 book New Bottles for New Wine.
As Klyczek wrote, Huxley argued that “the eugenic goals of biologically engineering human evolution should be refined through transhumanist technologies, which combine the eugenic methods of genetic engineering with neurotech that merges humans and machines into a new organism.”
Earlier, in 1946, Huxley noted in his vision for UNESCO that it was essential that “the eugenic problem is examined with the greatest care and that the public mind is informed of the issues at stake so that much that is now unthinkable may at least become thinkable,” an astounding statement to make so soon after the end of World War II.
Thanks in large part to the Wellcome Trust and its influence on both policy and medical research over the course of several decades, Huxley’s dream of rehabilitating eugenics-infused science in the post–World War II era could soon become reality. Unsurprisingly, the Wellcome Trust hosts the archive of the formerly Huxley-led Eugenics Society and still boasts close ties to its successor organization, the Galton Institute.
The over-riding question is: Will we allow ourselves to continue to be manipulated into allowing transhumanism and eugenics to be openly pursued and normalized, including through initiatives like those of Wellcome Leap that seek to use babies and toddlers as test subjects to advance their nightmarish vision for humanity?
If well-crafted advertising slogans and media campaigns painting visions of utopia such as “a world without disease” are all that is needed to convince us to give up our future and our children’s future to military operatives, corporate executives, and eugenicists, then there is little left of our humanity to surrender.